Colles' Fracture
- Article Author:
- Kevin Summers
- Article Editor:
- Sarah Fowles
- Updated:
- 8/10/2020 4:51:45 PM
- For CME on this topic:
- Colles' Fracture CME
- PubMed Link:
- Colles' Fracture
Introduction
Named after Abraham Colles, who first described a distal radius fracture in 1814 at the Royal College of Surgeons in Dublin, the Colles fracture is one of the most common fractures encountered in orthopedic practice. The Colles fracture is defined as a distal radius fracture with dorsal comminution, dorsal angulation, dorsal displacement, radial shortening, and an associated fracture of the ulnar styloid.[1] The term Colles fracture is often used eponymously for distal fractures with dorsal angulation.[2] These distal radius fractures are often caused by falling on an outstretched hand with the wrist in dorsiflexion, causing tension on the volar aspect of the wrist, causing the fracture to extend dorsally.
Etiology
The Colles fracture is most commonly caused by a fall, landing on an outstretched hand with the wrist in dorsiflexion. This condition is also known as a "fall on outstretched hand injury," referred to by the acronym "FOOSH injury." The severity of the injury is usually determined by the position of the wrist when injured as well as the amount of force of the trauma. Tension on the volar aspect of the wrist causes bending and compressive forces. As a result of these forces through the wrist, dorsal displacement and comminution occur.
Epidemiology
Distal radius fractures occur in people of all ages; however, they seem to mostly affect people in a bimodal distribution in two main populations: young athletes and the elderly. In pediatrics, fractures often occur around the time of puberty due to low bone mineralization. Young athletes, most commonly in boys and young men due to playing sports or other athletic activities, get these injuries after high impact trauma associated with sporting injuries. These ages, however, from about age 19 to 49 years old make up the least common age group for these injuries.[3] Elderly individuals, more commonly in women than men, sustain distal radius fractures due to falls associated with aging. Osteoporosis associated with aging increase the risk of these fractures in elderly individuals, and also increases risk in women, who are more commonly affected with osteoporosis.[4]
Pathophysiology
The most common cause of Colles fractures is trauma. In younger patients, this usually relates to athletic injuries or motor vehicle accidents. In the elderly population, this is most often caused by falls. When the traumatic force hits an outstretched hand, force is transmitted dorsally through the wrist, fracturing the distal radius, displacing it dorsally, and also often causing dorsal comminution as well. This mechanism leads to the classic “dinner fork” deformity of the wrist with associated pain, edema, and decreased range of motion.[5]
History and Physical
In distal radius fractures, thorough physical exams of the affected and nonaffected extremities are important in the diagnosis and management of the injury. Wrist pain and tenderness to palpation will present on the exam. A classic dorsiflexion deformity is often seen and is also known as a “dinner fork” deformity. Bruising and swelling may also be visible, and a thorough skin exam is necessary to evaluate for a possible open fracture. The range of motion may be decreased due to the injury but should be assessed by the clinician if possible. Neurovascular status of the extremity distal to the injury requires an assessment as well, including a full exam of pulses, sensation, and motor function of the affected extremity. Finally, joints above and below the injury always need to be assessed as well to evaluate for other associated injuries.
Evaluation
Radiographs are usually the mainstay of evaluation, diagnosis, and initial management of these injuries. PA and lateral views should be taken at a minimum to evaluate these injuries. These radiographs help to distinguish the type of injury among different types of forearm fractures to narrow down and make a diagnosis.[6]
When plain films appear normal, and injury is still suspected, CT may be used to evaluate for occult fractures.
MRI is not a recommended diagnostic measure as the initial evaluation; however, it may serve to assess ligamentous or soft tissue extents of these injuries.
Treatment / Management
After diagnosing a Colles fracture with imaging, the clinician should determine the amount of displacement, and the decision made whether or not immediate reduction is needed. The displaced fracture can usually be reduced with traction of the hand and counter traction at the elbow while applying volar/medial force to the distal radial fractured fragment. Pronation may also be needed to overcome the supination deformity. The injury should then be immobilized with a temporary sugar tong splint. The wrist will need reimaging with radiographs post-reduction, and the neurovascular status of the hand requires assessment after the splint is applied. The definitive treatment would then be to have the splint removed, and a forearm cast applied. After splinting or casting, the patient needs to be carefully instructed on “red flag” symptoms to watch for, which include severe pain, discoloration of fingers or nail beds, edema, numbness/tingling of the fingers, or decreased finger range of motion.
The majority of Colles fractures are manageable with casting and conservative management. Fractures that are unstable with significant displacement or comminution have demonstrated to have better outcomes with surgical management. Fractures that are unable to attain proper alignment with reduction may require percutaneous pinning to achieve ideal positioning. External fixation may be necessary for comminuted fractures that cannot be maintained in the appropriate positioning with a cast. Fractures with significant displacement and palmar dislocation of the carpus are very unstable and sometimes require internal fixation with pins and/or plates. After healing and cast removal, physical therapy can help to improve range of motion with muscle and ligament strengthening specifically for the injured hand and wrist affected.[7]
Differential Diagnosis
The differential diagnosis for Colles fractures includes other types of distal radius fractures, as well as other forearm fractures, each of which can be differentiated with radiographic imaging.
Smith fracture: Often referred to as a “reverse Colles,” the Smith fracture involves volar (rather than dorsal) angulation of the distal radial fragment, and is usually caused by a FOOSH in supination, rather than in pronation.
Barton fracture: A Barton fracture is another type of distal radius fracture that involves the dorsal rim of the distal radius, in which an oblique intra-articular fracture occurs.
Hutchinson or Chauffer fracture: Intra-articular radial styloid fractures are also known as Hutchinson or Chauffer fractures, and usually present as oblique or transverse fractures to the radial styloid caused by direct trauma.
Galeazzi fracture: Fracture of the medial or distal radius with associated dislocations of the distal radioulnar joint.[8]
Monteggia fracture: Ulnar shaft fracture with associated radial head dislocation.[9]
Essex Lopresti lesion: Rare combination of Galeazzi and Monteggia fractures, involving a radial head fracture at the elbow with associated DRUJ disruption at the wrist and interosseous membrane disruption throughout the forearm.
Prognosis
The prognosis of a Colles fracture depends on the severity of the injury and the extent of any complications that arise as a result of the injury. Complications are avoidable through prompt and adequate reduction followed by splinting and casting and follow-up with an orthopedist. Severe injuries such as an open fracture or injury with neurovascular compromise or evidence of compartment syndrome require urgent orthopedic consultation. Severe injuries often need surgical repair. Prognosis also depends on patient age, as younger patients have excellent potential for bone remodeling, while elderly patients are less likely to have such positive outcomes.[10]
Complications
Complications of Colles fractures can be classified as early and late and can range from mild effect to significant long-term disability. Dangerous early complications include compartment syndrome, median nerve injury, and vascular injury. Less acute and long-term complications include carpal tunnel syndrome and osteoarthritis. Malunion can occur when successful reduction does not hold. It can result in tendon injury and lead to chronic wrist pain.[11]
Deterrence and Patient Education
The patient's with wrist injuries concerning fractures should seek immediate medical attention. Colles fractures are one of the most common wrist injuries made up of a distal radius fracture with dorsal displacement. These injuries need prompt reduction followed by splinting and casting with follow up by an orthopedist to ensure proper healing. Severe injuries may require surgical repair. Patients need to be aware of the appropriate splint and cast management, involving the adequate assessment of neurovascular status. If a cast is too tight, causing severe pain, numbness or tingling of the fingers, or discoloration of the fingers, immediate medical attention is warranted. With proper treatment, management, and follow-up of these injuries, the anatomy is restorable, and good functional outcomes achieved.
Enhancing Healthcare Team Outcomes
Patients with Colles fractures frequently present for medical attention and require a complete interprofessional team for comprehensive and optimal management. For example, if a patient presents to an emergency department, they interact with various medical personnel to get the care they require. The orthopedic surgeon will often be the final destination for these patients, as this is often the optimal treatment to correct the injury, however they are usually not the patient's point of initial contact.[12] Patients will initially present to emergency departments, urgent care centers, or physician outpatient offices, where they will interact with intake triage nurses. The patient will then interact with patient care nursing staff, radiology technicians for imaging, possibly laboratory technicians if lab work is needed, and emergency physicians, or another physician in the office they have visited for treatment. The treatment team will often work together with radiologists reading the images to make the diagnosis. Orthopedic surgeons are usually contacted for treatment options following a confirmed diagnosis, as surgery is often necessary for definitive management depending on the severity of the injury. Communication among all aspects of the healthcare team is essential in ensuring proper care for the patient promptly. Physical and occupational therapists may have involvement after the removal of the cast. Orthopedic nurses will often assume the role of care coordinator, managing the contacts between PT, the surgeon, any potential pharmacy involvement for pain control at the initial injury, and assisting with reduction and surgery. These interprofessional measures can drive better outcomes for patients with a Colles fracture [Level 5]
(Click Image to Enlarge)

Colles, Wrist, X-ray
Contributed by Steve Bhimji, MS, MD, PhD
(Click Image to Enlarge)

Colles fracture
Image courtesy S Bhimji MD
(Click Image to Enlarge)
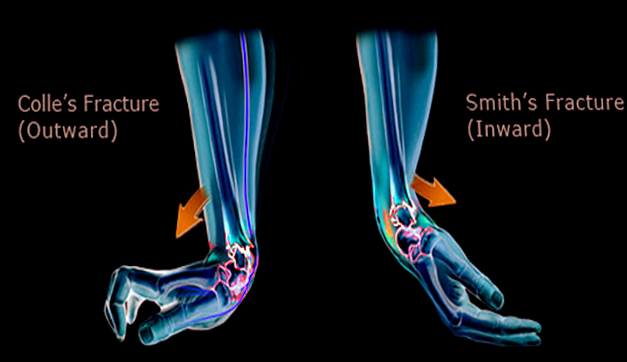
Smith vs Colles fracture
Image courtesy O.Chaigasame