Dementia
- Article Author:
- Prabhu Emmady
- Article Editor:
- Prasanna Tadi
- Updated:
- 8/10/2020 9:05:46 PM
- For CME on this topic:
- Dementia CME
- PubMed Link:
- Dementia
Introduction
Dementia is a disorder that is characterized by cognitive decline involving memory and at least 1 of the other domains, including personality, praxis, abstract thinking, language, executive functioning, complex attention, social and visuospatial skills.[1] In addition to the noted decline, the severity must be significant enough to interfere with daily functionality. It is often a progressive disorder, and individuals often do not have insight into their deficits. Currently, no cure exists for any of the causes of dementia. With improving outcomes from diseases like cancer and elongating lifespan, the incidence and prevalence of dementia are expected to continue to increase. Currently, 47 million people in the world have dementia, and the number is expected to triple by 2050.[2] Alzheimer disease is the 6th leading cause of death in the United States and the 5th leading cause in the world. Dementia is a significant public health burden and significantly increases costs of care, both to the individual and society. The individual lifetime cost to care for an individual with dementia was nearly $200,000 more than an individual without dementia.[3] In 2010, the costs of treating dementia in the United States were projected to be about $200 billion.[4]
Etiology
Several conditions cause dementia. Alzheimer dementia (AD) is the most common cause of dementia and accounts for about 70% of cases.[5] Other common causes dementia of include vascular dementia, dementia of Lewy bodies (DLB), frontotemporal dementia (FTD), and Parkinson disease dementia (PDD). Other diseases account for fewer cases of dementia, and these include Huntington disease (HD), cortical basal degeneration (CBD), progressive supranuclear palsy (PBP), multisystem atrophy (MSA), and Creutzfeldt-Jakob disease (CJD).
AD is caused by the deposition of neurofibrillary tangles and senile plaques in the brain.[6] Vascular dementia occurs due to ischemic injury to the brain.[7] Frontotemporal dementia is a disorder that is caused by various mutations leading to the deposition of tau protein and other proteins in the grey and white matter of the brain.[8] Lewy body dementia is caused by abnormal aggregation of the synaptic protein αlpha-synuclein in the brain.[9]
Epidemiology
Alzheimer disease (AD) is the most common cause of dementia, as it is responsible for 70 to 80% cases of all cases of dementia. It can occur sporadically or be familial.[6]
Vascular dementia (VD) accounts for 5% to 10 % of all dementia cases. Its incidence increases with age and doubles every 5 years. Risk factors for vascular dementia include hypercholesteremia, diabetes mellitus, hypertension, and smoking.[7]
Lewy body dementia (LBD) accounts for 5% to 10% of cases of dementia. The epidemiological data may not be completely accurate because the diagnosis of Lewy boy dementia is often missed.[10]
Frontotemporal dementia (FTD) is the second most common cause of dementia in patients less than 65 years of age. 25% of all dementia cases in patients above the age of 65 are attributed to frontotemporal dementia. There are, however, many limitations in the epidemiological studies of frontotemporal dementia.[8]
Creutzfeldt-Jakob disease (CJD) is very rare and occurs in about 1 in a million.
Mixed dementia is a condition in which patients have more than 1 type of dementia. In this condition, AD with LBD or vascular dementia are the most common coexistent dementias.[11]
Pathophysiology
The pathophysiology of dementia is not understood completely. Most types of dementia, except vascular dementia, are caused by the accumulation of native proteins in the brain.
Alzheimer disease is characterized by widespread atrophy of the cortex and deposition of amyloid plaques and tangles of hyperphosphorylated tau protein in the neurons which contribute to their degeneration. Lewy body dementia is characterized by the intracellular accumulation of Lewy bodies (which are insoluble aggregates of alpha-synuclein) in the neurons, mainly in the cortex. Frontotemporal dementia is characterized by the deposition of ubiquitinated TDP-43 and hyperphosphorylated tau proteins in the frontal and temporal lobes leading to dementia, early personality, and behavioral changes, and aphasia. Vascular dementia is caused by ischemic injury to the brain (e.g., stroke), leading to permanent neuronal death.[7]
A genetic basis has been established for both early and late-onset AD. Certain factors like depression, traumatic head injury, cardiovascular disease, family history of dementia, smoking, and the presence of APOE e4 allele have been shown to increase the risk of development of AD.
Histopathology
Alzheimer disease: Protein deposits can be seen on histopathological studies of the brain in patients with Alzheimer dementia. Different immunohistochemical stains are used to identify the protein deposits in the brain. Dense core and diffuse plaques are seen in the neurons. Dot-like deposition of ubiquitin is seen on histopathology of the brain in patients with frontotemporal dementia.[12]
In Lewy body dementia, there are neuronal cytoplasmic depositions of Lewy bodies. These are formed of ubiquitin and alpha-synuclein.[13]
Neurodegeneration and vascular changes are seen in the brains of patients with vascular dementia.[14]
History and Physical
History must be obtained from the patient and their family members. Patients may present with symptoms of change in behavior, getting lost in familiar neighborhoods, memory loss, mood changes, aggression, social withdrawal, self-neglect, cognitive difficulty, personality changes, difficulty performing tasks, forgetfulness, difficulty in communication, vulnerability to infections, loss of independence, etc., A detailed history should include past medical, family, drug, and alcohol history.
In addition to symptoms of dementia, the following atypical symptoms may be seen in the following conditions:
- In patients with LBD, symptoms of well-formed visual hallucinations, delusions, sleep disturbances, and trouble processing visual information can be seen.
- In patients with CJD, symptoms of muscle stiffness, twitches, muscle jerks, visual hallucinations, and double vision may be seen.
- In patients with Huntington disease, symptoms of chorea, irritability, and obsessive-compulsive behavior may be seen.
- In patients with vascular dementia, symptoms of imbalance, headache, sensorimotor deficits, and speech difficulties may be seen.
- In patients with FTD, behavior changes, problems with spatial orientation, and speech difficulties may be seen.
- In patients with PDD, symptoms of parkinsonism characterized by muffled speech, slow movement, tremors may be seen. In addition, visual hallucinations and delusions may also be seen, especially in the late stages.
Patients with MSA, PSP, and CBD have symptoms of parkinsonism. In addition, MSA has symptoms of autonomic failure, PSP has symptoms of blurry vision and difficulty controlling eye movement, CBD has progressive asymmetric muscle rigidity and myoclonus.
Evaluation
The definitive diagnosis of the type of dementia can only be made at autopsy. Clinical history is a very important aspect in the evaluation of a patient with dementia. Work up must include laboratory testing to evaluate for treatable causes of cognitive impairment.
A comprehensive physical and neurological examination must be performed. All domains of cognition must be assessed. Mini-mental status examination (MMSE) can help in evaluating attention, orientation, language, memory, and visuospatial skills. MMSE is not diagnostic of dementia and cannot differentiate between dementia and other treatable causes of dementia.[15] Alternatives to MMSE include Montreal Cognitive Assessment (MoCA), Addenbrooke's Cognitive Examination–Revised (ACE-R), the modified mini-mental state examination, Mini-Cog, and Rowland Universal Dementia Assessment Scale (RUDAS). These tests are to be used as a screening test, and they can also help in monitoring disease progression. In the dementia clinic setting, MMSE was noted to have a sensitivity of 85.1% and specificity of 85.5%, while the sensitivity was in 71.1%, and specificity was 95.6% in the mixed specialist hospital setting.[16]
Laboratory tests to be considered in all patients in the evaluation of dementia include complete blood count, urinalysis, metabolic panel, B12, folic acid, Thyroid function tests, serological tests for syphilis. Additional work up to be considered when symptoms are atypical for Alzheimer dementia include erythrocyte sedimentation rate, electroencephalography (EEG), magnetic resonance imaging (MRI) of the brain, lumbar puncture, heavy metal screen, ceruloplasmin levels, Lyme disease titer, human immunodeficiency virus (HIV) screening, serum protein electrophoresis, etc.,
Formal neuropsychological testing can help with the establishment of the diagnosis and social decision making as the disease advances. These have high sensitivity and specificity. They can help evaluate the extent and severity of cognitive impairment as well as behavioral impairments. They can help differentiate normal aging from mild cognitive impairment and identify the type of dementia.
Functional brain imaging with PET, SPECT, and fMRI can help in early diagnosis and monitoring of patients with dementia, especially AD. These can also help differentiate the etiology of dementia. These are expensive and routine use in clinical practice is not indicated.
CJD: The diagnosis of CJD is established by the presence of rapidly progressive dementia and the presence of at least 2 of the 4: myoclonus, akinetic mutism, pyramidal/extrapyramidal signs, and visual/cerebellar signs. CJD has unique abnormalities in diagnostic testing, and these can help in confirming the diagnosis. Periodic sharp-wave complexes at 1 Hz frequency are characteristic EEG findings seen in this condition, though other findings like diffuse slowing and frontal rhythmic delta activity. MRI may show T2 hyperintensity in the basal ganglia, thalamus, and cortex. 14-3-3 is positive in CSF testing.[17]
Treatment / Management
FDA approved medications to improve cognitive functions include cholinesterase inhibitors and memantine. Cholinesterase inhibitors are donepezil, galantamine, and rivastigmine. Cholinesterase inhibitors prevent the breakdown of acetylcholine and can slow or delay the worsening of symptoms. Memantine is an NMDA agonist and decreases the activity of glutamine. Donepezil is approved for all stages of Alzheimer disease, galantamine, and rivastigmine for mild to moderate stage and memantine for moderate to severe stage.[18]
Behavior symptoms include irritability, anxiety, and depression. Antidepressants like SSRI, antipsychotics, and anxiolytics can help with these symptoms. In addition, non-drug approaches like supportive care, memory training, physical exercise programs, mental and social stimulation must be employed in symptom control.
Treatment of sleep symptoms must be an important consideration in patients with dementia. Medication options include amitriptyline, lorazepam, zolpidem, temazepam, quetiapine, etc., Non-drug approaches include daily exercise, light therapy, sleep routine, avoiding caffeine and alcohol, pain control, biofeedback, and multicomponent cognitive-behavioral therapy.[19]
There are many other drugs that are still under investigation, such as anti-tau protein agents.[12] So far, these have not shown promising results.
Patients and their families should be counseled about the disease and its consequences. They should be provided with all the necessary information in regards to what to expect and how to react to it. Patients and their families should also be encouraged to seek social service consultations and to register with support groups and societies such as the Alzheimer society. Driving restrictions may have to be imposed.
Differential Diagnosis
- Delirium
- Depression
- Drug use
- Normal age-associated memory changes
- Mild cognitive impairment
- Stress
- Structural brain abnormalities like subdural hematoma, brain tumor, and normal pressure hydrocephalus
- Infections like HIV, neurosyphilis
- Thiamine deficiency
- Vitamin B12 deficiency
- Folic acid deficiency
- Thyroid disorders
- Metabolic abnormalities and derangements
- Medication-induced
- Vitamin E deficiency
Prognosis
The prognosis with dementia is poor. Dementia is often a progressive condition with no cure or treatment. 1-year mortality rate was 30-40% while the 5-year mortality rate was 60-65%. Men had a higher risk than women. Mortality rates among admitted patients with dementia was higher than those with cardiovascular diseases.[20]
Complications
Dementia can affect many body systems and can lead to the following complications:[21]
- Inadequate nutrition
- Pneumonia
- Inability to perform self-care tasks
- Personal safety challenges
- Fractures due to falls
- Hallucinations and Delusions
- Apathy
- Agitation
- Dysphagia
- Death
- Depression
- Incontinence
- Personality changes
- Infections
Deterrence and Patient Education
The diagnosis of dementia can be stressful and overwhelming for the patients and their families. Patient education must be an important part of the clinical management of patients with dementia. Counseling must be given about regular clinic visits about medication compliance, a healthy diet, exercise, and sleep hygiene. Support groups can help with the reduction of issues like anxiety, frustration, anger, loneliness, and depression. The patient should be counseled about the diagnosis and the prognosis. Creating an individualized care plan can empower the patient.
Enhancing Healthcare Team Outcomes
Dementia is a common condition, and its prevalence is expected to increase with time. It is caused by various diseases, and each of them may present differently. An interprofessional approach is recommended when managing patients with dementia. Interventions like care coordination and interprofessional communication can help reduce hospitalization and decrease emergency department visits.
Physicians must coordinate with other healthcare workers, including other physicians, pharmacists, nurses, when managing patients with dementia. Any medication change must be carefully coordinated with all physicians involved in the patient's care. Pharmacists can help with counseling about medication side effects and compliance. Safety in the current living situation must be reviewed during every clinic visit, and social workers must be consulted to investigate and coordinate safety-related incidents. Involving family members and caregivers is an important aspect in the care of patients with dementia. They must be encouraged to accompany the patient during clinic visits to provide an accurate clinical history and to reiterate the plan. They can also help decrease the likelihood of no shows, which can be an issue in patients with dementia.
(Click Image to Enlarge)
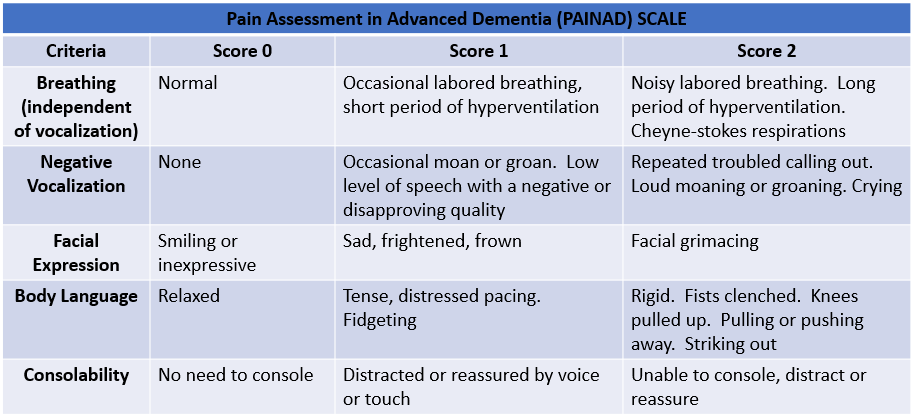
Pain Assessment in Advanced Dementia (PAINAD) SCALE
Contributed by Daniel Schwerin, MD, FACEP, FAEMS, FAAEM