Dengue Fever
- Article Author:
- Timothy Schaefer
- Article Author:
- Prasan Panda
- Article Editor:
- Robert Wolford
- Updated:
- 8/23/2020 9:42:42 PM
- For CME on this topic:
- Dengue Fever CME
- PubMed Link:
- Dengue Fever
Introduction
Dengue is a mosquito-transmitted virus and the leading cause of arthropod-borne viral disease in the world. It is also known as breakbone fever due to the severity of muscle spasms and joint pain, dandy fever, or seven-day fever because of the usual duration of symptoms. Although most cases are asymptomatic, severe illness and death may occur. Aedes mosquitoes transmit the virus and are common in tropical and subtropical parts of the world. The incidence of dengue has increased dramatically over the past few decades. The infection is now endemic in some parts of the world. A few people who were previously infected with one subspecies of the dengue virus develop severe capillary permeability and bleeding after being infected with another subspecies of the virus. This illness is known as dengue hemorrhagic fever.[1][2][3]
Etiology
Epidemiology
It is the fastest spreading mosquito-borne viral disease in the world, affecting greater than 100 million humans annually. Dengue also causes 20 to 25,000 deaths, primarily in children, and is found in more than 100 countries. Epidemics occur annually in the Americas, Asia, Africa, and Australia. Two transmission cycles maintain the dengue virus: 1) mosquitos carry the virus from a non-human primate to a non-human primate and 2) mosquitos carry the virus from human to human. The human-mosquito cycle occurs primarily in urban environments. Whether the virus transmits from human to mosquito is dependent upon the viral load of the mosquito’s blood meal.
The primary vectors of the disease are female mosquitoes of the species Aedes aegypti and Aedes albopictus. Although A. aegypti is associated with most infections, A. albopictus’ range is expanding and may be associated with increasing numbers. These species of mosquitoes tend to live indoors and are active during the day. Transmission perinatally, via blood transfusions, breast milk, and by organ transplantation have been reported.
After 2010, the mean age of patients was 34 years as compared to 27.2 years from 1990 to 2010. The dengue viral serotype causing disease outbreaks has varied with time, as has the occurrence of severe dengue fever.[7][8]
Pathophysiology
Part of the Flavivirus family, the dengue virus is a 50 nm virion with three structural and seven nonstructural proteins, a lipid envelope, and a 10.7 kb capped positive sense single strand of ribonucleic acid. Infections are asymptomatic in up to 75% of infected humans. A spectrum of disease, from self-limiting dengue fever to hemorrhage and shock, may be seen. A fraction of infections (0.5% - 5%) progress to severe dengue. Without proper treatment, fatality rates may exceed 20%. These occur primarily in children. The typical incubation period for the disease is 4 to 7 days, but it can last from 3 to 10 days. Symptoms more than two weeks after exposure are unlikely to be due to dengue fever.
The exact course of events following the dermal injection of dengue virus by a mosquito bite is unclear. Skin macrophages and dendritic cells appear to be the first targets. It is thought that the infected cells then move to the lymph nodes and spread through the lymphatic system to other organs. Viremia may be present for 24 to 48 hours before the onset of symptoms. A complex interaction of host and viral factors then occurs and determines whether the infection will be asymptomatic, typical, or severe. Severe dengue fever with increased microvascular permeability and shock syndrome is thought to be associated with infection due to a second dengue virus serotype and the patient's immune response. However, cases of severe dengue do occur in the setting of infection by only a single serotype. Worsening microvascular permeability often transpires even as viral titers fall.
History and Physical
The three phases of dengue include febrile, critical, and recovery.
During the febrile phase, a sudden high-grade fever of approximately 40 C occurs that usually lasts two to seven days. Associated symptoms include facial flushing, skin erythema, myalgias, arthralgias, headache, sore throat, conjunctival injection, anorexia, nausea, and vomiting. For skin erythema, a general blanchable macular rash occurs in the first one to two days of fever and the last day of fever. Or, within 24 hours, a secondary maculopapular rash can develop.
Defervescence characterizes the critical phase with a temperature of approximately 37.5 C to 38 C or less on days three through seven. It is associated with increased capillary permeability. This phase usually lasts one to two days. It can progress to shock, organ dysfunction, disseminated intravascular coagulation, or hemorrhage.
The recovery phase entails the gradual reabsorption of extravascular fluid in two to three days. The patient will display bradycardia at this time.
Evaluation
Common laboratory findings include thrombocytopenia, leukopenia, elevated aspartate aminotransferase. The disease is classified as dengue or severe dengue. [9][10][11]
Criteria for Dengue Include:
- Probable dengue: The patient lives in or has traveled to a dengue-endemic area. Symptoms include fever and two of the following: nausea, vomiting, rash, myalgias, arthralgias, rash, positive tourniquet test, or leukopenia.
- Warning Signs of Dengue: Abdominal pain, persistent vomiting, clinical fluid accumulation such as ascites or pleural effusion, mucosal bleeding, lethargy, liver enlargement greater than 2 cm, increase in hematocrit, and thrombocytopenia.
- Severe Dengue: Dengue fever with severe plasma leakage, hemorrhage, organ dysfunction including transaminitis greater than 1000 international units per liter, impaired consciousness, myocardial dysfunction, and pulmonary dysfunction.
- Dengue shock syndrome clinical warnings: Symptoms include rapidly rising hematocrit, intense abdominal pain, persistent vomiting, and narrowed or absent blood pressure.
The virus antigen can be detected by ELISA, polymerase chain reaction, or isolation of the virus from body fluids. Serology will reveal a marked increase in immunoglobulins.
It is vital to assess pregnant patients with dengue as the symptoms may be very similar to preeclampsia.
Treatment / Management
Supportive management includes giving the patient fluids, acetaminophen for fever, and a blood transfusion for hemorrhage. Confirmed diagnosis is established by culture, antigen detection, polymerase chain reaction, or serologic testing. Avoid giving aspirin and nonsteroidal anti-inflammatory drugs and other anticoagulants. No antiviral medications are recommended.
Patients with thrombocytopenia or bleeding may require platelets and fresh frozen plasma.
No laboratory tests can predict the progression to severe disease.
Differential Diagnosis
The clinical diagnosis of dengue can be challenging as many other illnesses can present similarly early in the disease course. Other considerations should include malaria, influenza, Zika, chikungunya, measles, and yellow fever. Obtain a detailed history of immunizations, travel, and exposures.
Rapid laboratory identification of dengue fever includes NS1 antigen detection and serologic tests. Serologic tests are only useful after several days of infection and may be associated with false positives due to other flavivirus infections, such as yellow fever or Zika virus.
Prognosis
Untreated severe dengue fever may have a mortality rate of 10% to 20%. Appropriate supportive care reduces the mortality rate to roughly 1%.
Complications
- Liver injury
- Cardiomyopathy
- Pneumonia
- Orchitis
- Oophoritis
- Seizures
- Encephalopathy
- Encephalitis
Postoperative and Rehabilitation Care
Patients should be encouraged to consume ample liquids. The return of a patient's appetite is a sign that the infection is subsiding.
Consultations
Consulting an infectious disease specialist is recommended because most clinicians have little experience managing this infection. The Centers for Disease Control and Prevention has a hotline which also offers advice on treatment.
Deterrence and Patient Education
The only way to avoid contracting dengue is to prevent mosquito bites and not travel to its endemic areas.
Other preventative measures include the use of DEET insecticide, wearing protective clothing, sleeping under a mosquito net, and eliminating stagnant water around the home.
Enhancing Healthcare Team Outcomes
The diagnosis and management of dengue is complex and this best managed by an interprofessional team that includes an infectious disease expert, CDC consultant, emergency department physician and an internist. The care is supportive with fluid, acetaminophen for fever, and a blood transfusion for hemorrhage. Confirmed diagnosis is established by culture, antigen detection, polymerase chain reaction, or serologic testing. No laboratory tests can predict the progression to severe disease.
The role of the primary care provider and nurse practitioner is to educate the traveler on the prevention of mosquito bites. This means covering exposed skin, and use bed nets, particularly during daytime siestas, using mosquito repellents and indoor insecticides. One should also eradicate mosquito breeding grounds like standing water. The prognosis for untreated dengue is abysmal but with supportive care, most patients can survive, albeit with residual multisystem organ damage.[12][13]
(Click Image to Enlarge)
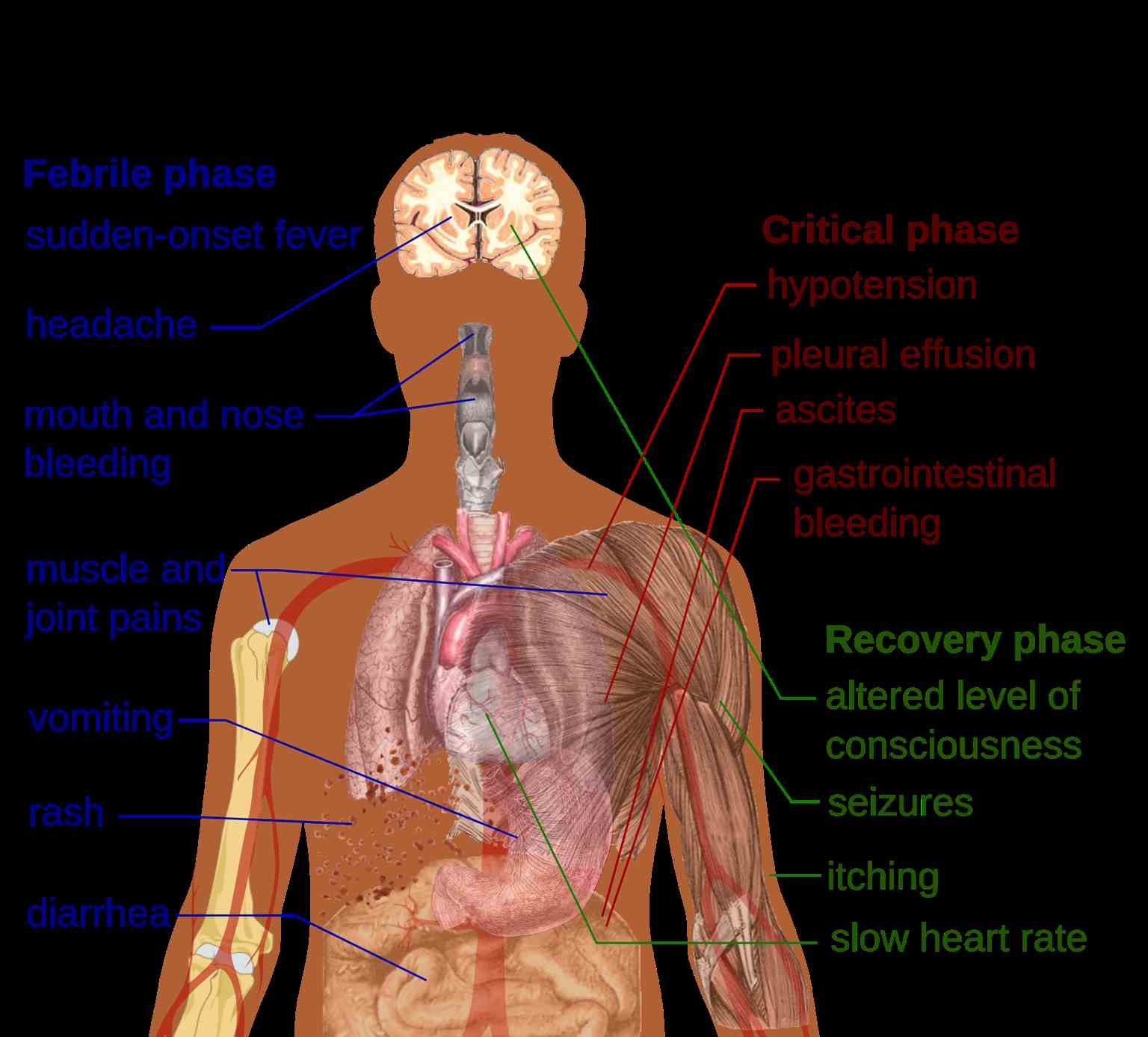
Main symptoms of dengue fever
Contributed by Wikimedia Commons (Public Domain)
(Click Image to Enlarge)

Mosquito carried diseases, Zika virus, Dengue fever, West Nile Fever, Chikungunya, Yellow Fever, Malaria
Contributed by National Institutes of Health (NIH)