Dermatofibroma
- Article Author:
- David Myers
- Article Editor:
- Eric Fillman
- Updated:
- 11/6/2020 7:35:10 AM
- For CME on this topic:
- Dermatofibroma CME
- PubMed Link:
- Dermatofibroma
Introduction
Dermatofibroma is a commonly occurring cutaneous entity usually centered within the skin's dermis. Dermatofibromas are referred to as benign fibrous histiocytomas of the skin, superficial/cutaneous benign fibrous histiocytomas, or common fibrous histiocytoma. These mesenchymal cell lesions of the dermis clinically are firm subcutaneous nodules that occur on the extremities in the vast majority of cases and may or may not be associated with overlying skin changes. They are most commonly asymptomatic and usually relatively small, less than or equal to 1 centimeter in diameter. The term "fibrous histiocytoma" refers more to the morphologic appearance of the cell populations that comprise these lesions rather than strictly describing the cellular lineage.
There are two theories of the genesis of dermatofibromas: (1) reactive process vs. a clonal, and (2) neoplastic proliferation. Evidence exists for both of these theories. Often, patients who present with a dermatofibroma relate a history of possibly inciting local trauma at the site, such as from an insect bite or superficial puncture wound from thorns or wood splinters. Dermatofibromas occur in people of all ages, although more commonly during the ages of the 20s to 40s, and develop more frequently in females than males, with as high as a 2:1 female to male predominance according to some reports. They are a benign tumor, although there have been cases of local recurrence, and even more rarely, distant metastases have been reported. When considering the differential diagnosis of these lesions, it is vitally important to distinguish dermatofibromas from dermatofibrosarcoma protuberans, a similar-appearing but more aggressive cutaneous neoplasm.[1][2][3][4]
Etiology
The development of dermatofibromas remains a controversial topic. Patients who are diagnosed with dermatofibroma often endorse a history of local trauma. This history argues for a reactive process. However, this history of local trauma is not reliably reported and only found in about a fifth of cases. More often, there is no inciting event or trauma, and the dermatofibroma develops spontaneously. Interestingly, although they will develop spontaneously, spontaneous regression is not commonly observed, which may support an argument against a primarily reactive process in favor of a clonal or neoplastic model.
Some studies have identified clonal markers in dermatofibromas cells by analyzing X-chromosome inactivation, which argues for a monoclonal pattern, and possibly favors a neoplastic process as the origin of development for dermatofibromas. Others propose that dermatofibromas are heterogeneously derived. They represent both a reactive and neoplastic process within the same lesion, wherein the histiocytoid component may be neoplastic, and the fibrous portion may result from reactive fibroblastic proliferation.
Most dermatofibromas occur as solitary lesions, only clinically presenting as multiple simultaneous lesions in 10% of cases. Interestingly, although there are multiple histologic benign variants of dermatofibromas, in patients with two or more simultaneously occurring dermatofibromas, the lesions tend to appear histopathologically similar.[5][6][4]
Epidemiology
Dermatofibromas are a common skin lesion in almost all populations, with one study reporting that they account for 3% of all dermatopathology laboratory specimens. The overall worldwide incidence is difficult to determine, as the vast majority of patients are asymptomatic, and therefore many patients may never seek care for these lesions. These lesions are most common in patients in their 20s to their 40s. Most studies indicate a female predominance, with an incidence ranging from equivocal to only slightly higher in females too as high as twice as frequent in females than males.[5][6][4]
Histopathology
Dermatofibromas have many histologic variants, including cellular, epithelioid, lipidized, aneurysmal, monster cell, and atypical (to name only a few), but the most frequently diagnosed is the common fibrous histiocytoma or common dermatofibroma.
The common dermatofibroma is characterized histopathologically by a localized proliferation of spindle-shaped fibrous cells admixed with histiocytoid cells within the dermis. This proliferation is usually nodular in appearance, with spiculated but moderately defined borders that may have a pushing appearance regarding the surrounding tissue. The spindle cells will form focally what is referred to as a “storiform” pattern, which describes a multi-centric whorling appearance of the elongated nuclei. There may be intermixed capillaries and lymphocytes or multinucleated giant cells. These proliferations are usually contained within the dermis, but it is not uncommon to observe a small portion of the lesion dipping down into the subcutaneous tissue along septal lines. A helpful and distinguishing characteristic is the presence of trapped collagen bundles or “collagen balls” within and between the fascicles of spindled fibrous cells. These entrapped collagen collections are more commonly found forming at the periphery of the lesion.
The overlying epidermis is usually separated by a clearly delineated and unaffected zone of separation, the "Grenz zone." Typical reactive epidermis changes include hyperkeratosis and acanthosis. The epidermis will also often exhibit elongated rete ridges diving into the dermis with hyperpigmented basal keratinocytes, referred to as the “dirty feet” sign.
Arguably the most important entity to distinguish dermatofibromas from is the similar-appearing, but much more worrisome, dermatofibrosarcoma protuberans (DFSP). These lesions are typically much more cellular, have marked storiform pattern, invade and involve the subcutis deeply, often entrapping fat as it dives and proliferates along the subcutaneous septae.[7][8][9]
History and Physical
Dermatofibromas are slow-growing lesions that can affect any part of the body but have a predilection for the extremities. Clinically these lesions are firm, non-tender cutaneous nodules, with or without overlying skin changes (such as tan-pink to reddish-brown discoloration, depending on the age of the lesion) with a smooth surface. Dermoscopic evaluation of these lesions will most commonly exhibit a central white patch with a peripheral pigmented network. Dermatofibromas are usually less than or equal to one centimeter in diameter. Patients are usually asymptomatic but will relate a history of local trauma at the site of the lesion, such as vaccination or an insect bite in approximately one out of five cases. A thorough full-body skin exam is important as these lesions may be subtle and are multiple in 10% of cases. The “dimple sign” is a characteristic finding where lateral inward digital pressure of the skin produces a central dimpling over the lesion.[8][9]
Evaluation
The most important evaluation is biopsy with histopathologic examination. These lesions can be reliably diagnosed through this method, along with the correlated clinical exam. If these lesions are evaluated before biopsy by sonography, they should appear as an avascular lesion within the dermis, which will often have superficial subcutis involvement and spiculated margins that are not well defined. The size and margins of these lesions correlate well on the histopathologic exam with sonographic findings.[10][11][12]
Treatment / Management
Dermatofibromas are benign lesions with excellent prognosis that are usually cured through surgical excision. In excisional biopsies with cellular or atypical variants, re-excision may be recommended to ensure clear margins because of the documented, albeit low, rate of local recurrence. Metastases are extremely rare but have been observed. No histopathologic appearance has been reliably indicated in which lesions will tend to recur or metastasize.[13][3]
Differential Diagnosis
There are many benign variants of dermatofibroma, which are not discussed here. It is more important to differentiate benign dermatofibromas from more advanced and aggressive neoplasms that may appear similar to dermatofibromas in some cases.
Dermatofibrosarcoma protuberans (DFSP) is a low to intermediate grade, locally aggressive neoplasm that can be mistaken for a benign dermatofibroma. Thankfully, there are several distinguishing features. DFSP is characteristically more cellular and will involve more of the subcutis, displaying “honeycomb” entrapment of subcutaneous fat. In difficult cases, immunohistochemical staining can be very helpful, as DFSP characteristically stains positive for CD-34 and will be factor XIIIa negative. Benign dermatofibromas will stain strongly positive for factor XIIIa but negative for the marker CD-34. Dermatofibromas may also show higher positive staining for D2-40. Ki-67 staining should indicate a much higher proliferation index in DFSP’s, and the mitotic rate should also be much higher in DFSP than in dermatofibromas. DFSPs are also often much larger lesions, with average diameters of 5 centimeters, according to one study.
Kaposi Sarcoma, also composed of a spindled cell proliferation within the dermis, may be mistaken for the aneurysmal variant of dermatofibroma as Kaposi Sarcoma characteristically displays red blood cells between spindled cellular areas and vascularity. However, Kaposi Sarcoma should display HHV-8 positivity and may also stain positive for CD31, CD34, and D2-40.
Basal cell carcinomas (BCC) can mimic a dermatofibroma with overlying follicular induction, which refers to epidermal hyperplasia such as basaloid proliferation. This differentiation is usually most difficult in superficial biopsies, which miss the underlying dermatofibroma. There may even be peripheral palisading in these lesions, a characteristic finding usually of BCCs. Important differentiating factors include the presence of CK20 positive Merkel cells in follicular induction. Other signs arguing for dermatofibroma may include clear cell hyperplasia, the absence of nuclear atypia, and crowding.[14][7][15][13]
Prognosis
Dermatofibromas are benign lesions with excellent prognosis. Some lesions even undergo spontaneous regression, which may lead to hypopigmented skin. Most dermatofibromas will remain static for years. With thorough excision, these lesions rarely recur, and only the most aggressive varieties show local recurrence in approximately 20% of patients. These lesions rarely metastasize.[16]
Complications
Complications of dermatofibroma are primarily related to surgical removal, including bleeding, infection, scar/disfigurement, and need for further procedures.
Deterrence and Patient Education
Patients should be educated that dermatofibromas are benign entities and do not necessarily require excision. However, although the clinical history and exam and imaging studies may favor a dermatofibroma, a definitive diagnosis can only be made on pathologic examination. Patient requests or desires may also influence the decision to excise vs. choosing surveillance.
Enhancing Healthcare Team Outcomes
Patients should be educated that dermatofibromas are benign entities and do not necessarily require excision. However, although the clinical history and exam and imaging studies may favor a dermatofibroma, a definitive diagnosis can only be made following pathologic examination. Patients may also influence the decision to excise versus choosing surveillance. Of course, if surveillance is opted for, any abrupt or unusual change in the behavior of any skin lesion should necessitate a referral to a competent dermatologist for evaluation. [Level 4]
(Click Image to Enlarge)

Dermatofibroma
Contributed by DermNetNZ
(Click Image to Enlarge)
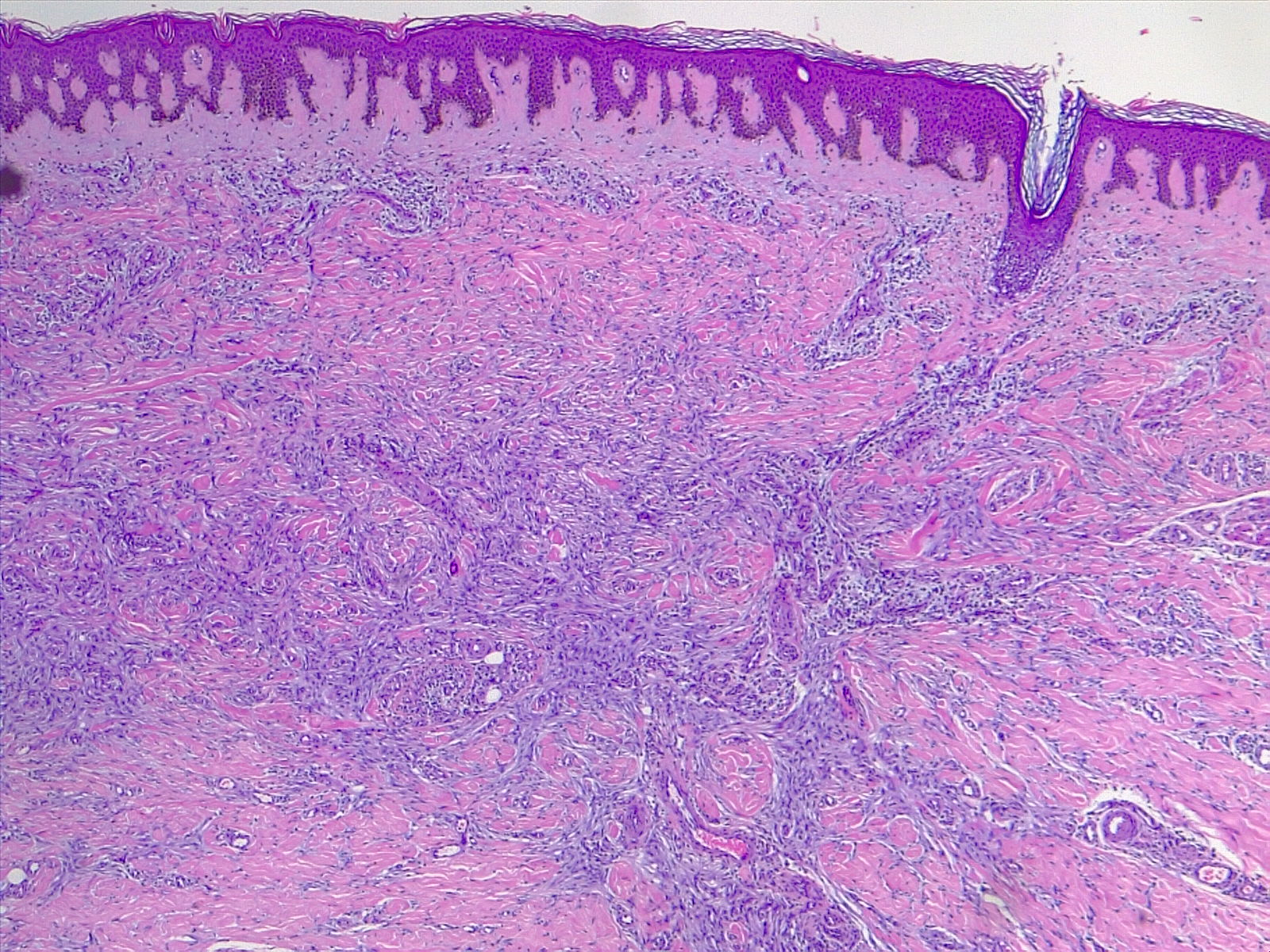
Dermatofibroma, H/E 4x. Low power view of a dermal proliferation of spindle cells entrapping collagen bundles.
Contributed by Fabiola Farci, MD
(Click Image to Enlarge)
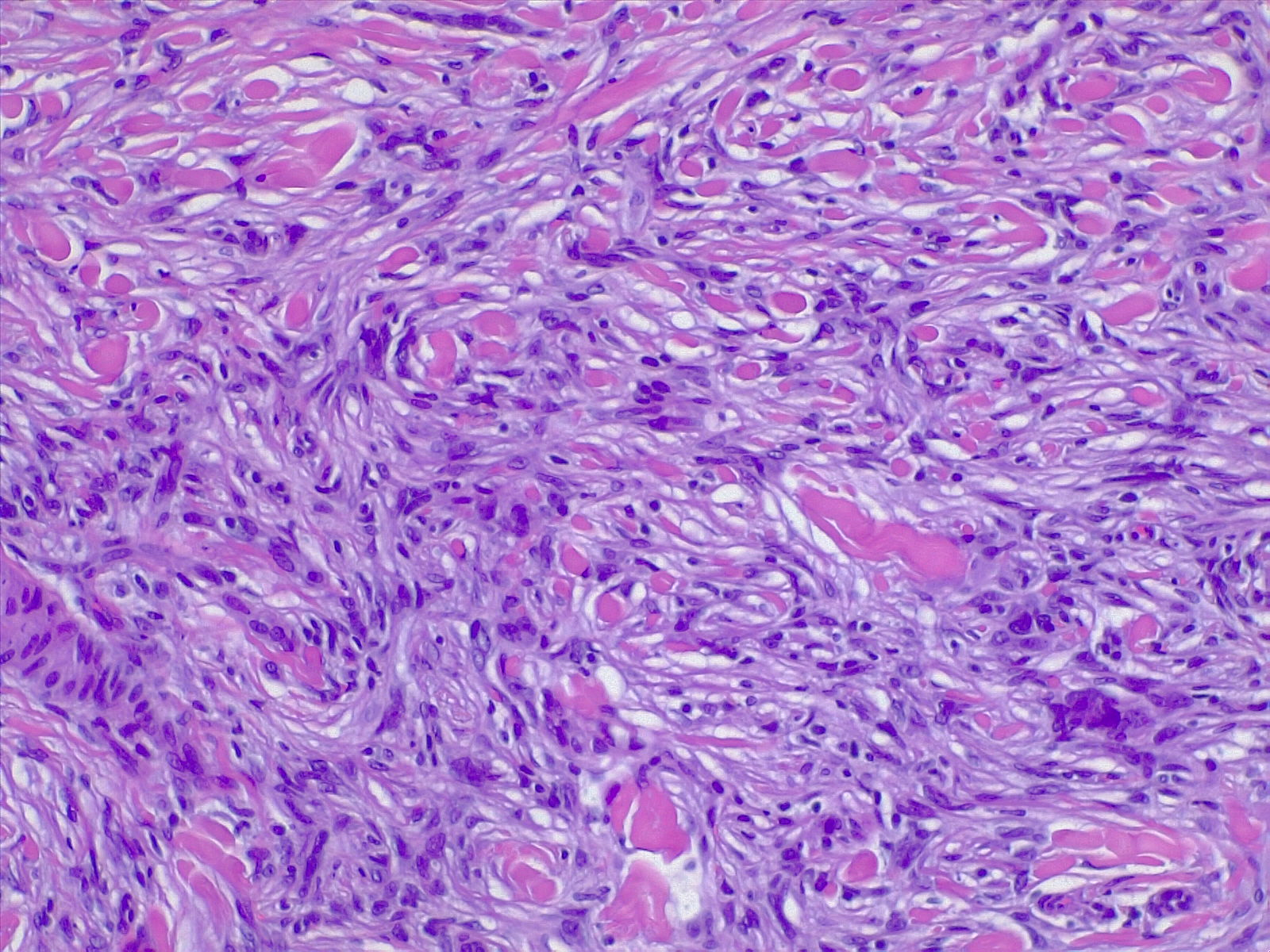
Dermatofibroma H/E 10x. Spindle cells entrapping collagen bundles.
Contributed by Fabiola Farci, MD
(Click Image to Enlarge)
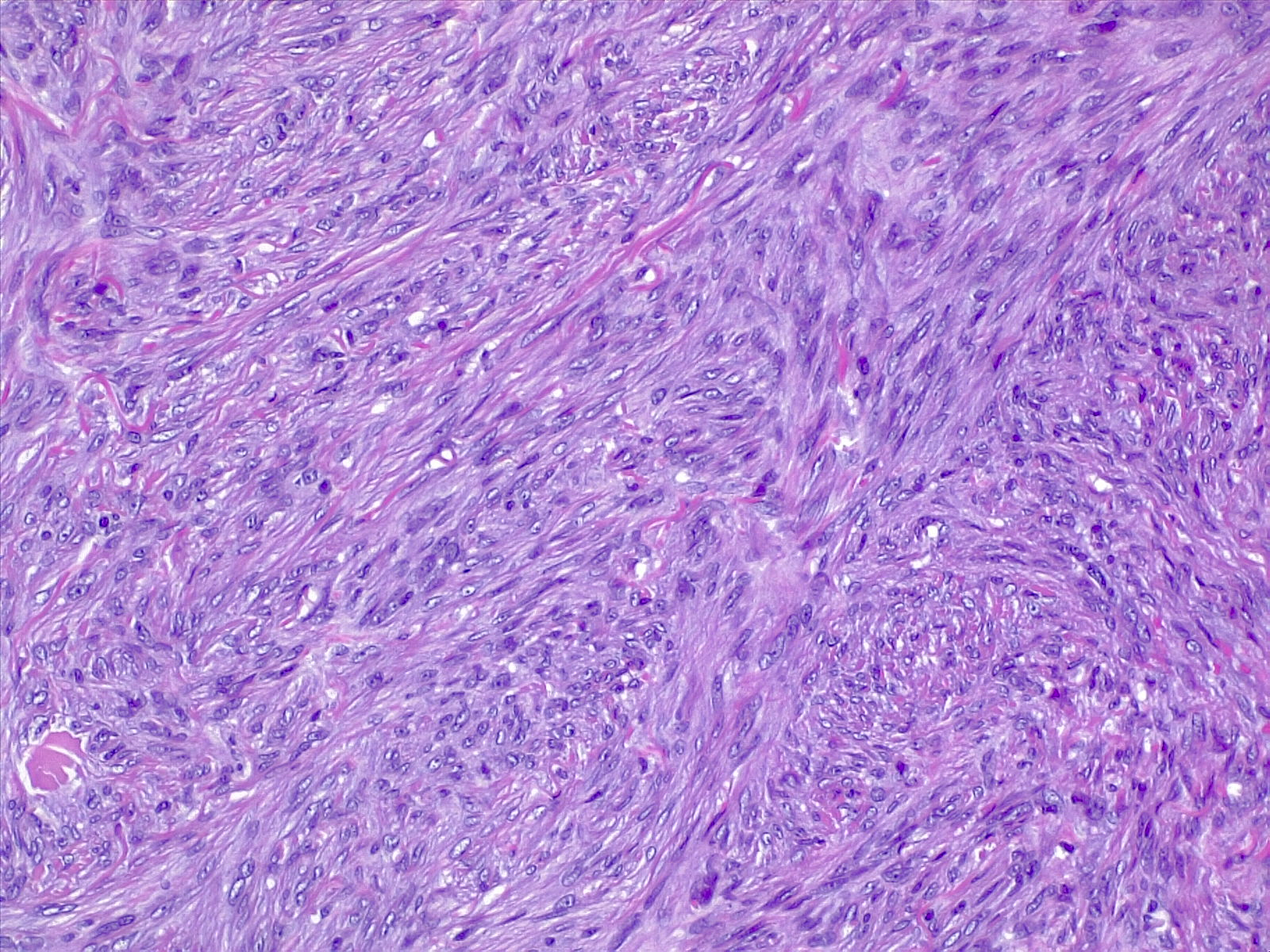
Spindle cells with bland nuclear features, disposed in short fascicles. H/E stain.
Contributed by Fabiola Farci, MD
(Click Image to Enlarge)
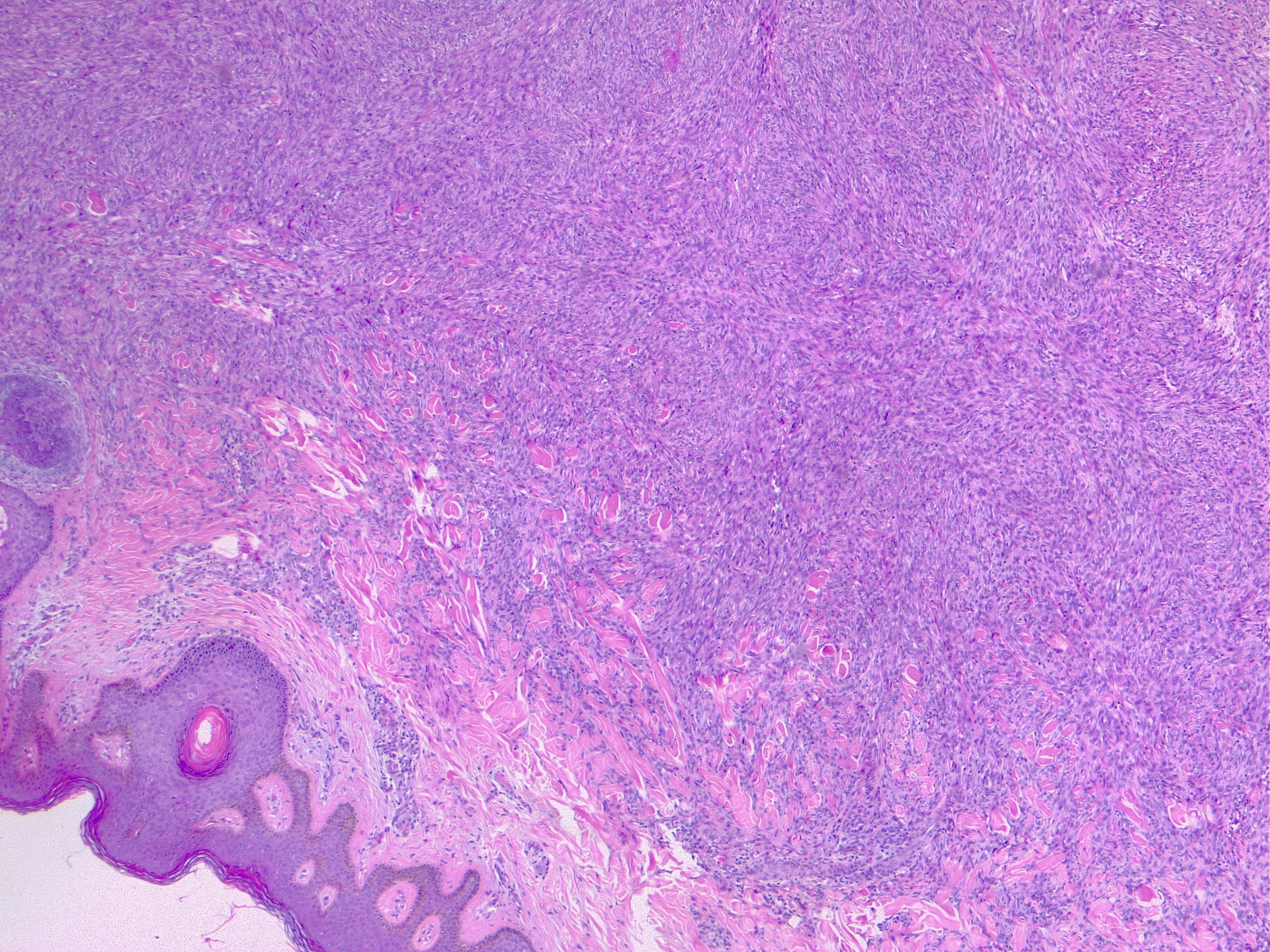
Cellular dermatofibroma, also known as cellular fibrous histiocytoma. H/E 4x.
Contributed by Fabiola Farci, MD