Diaphragmatic Hernia
- Article Author:
- Kayleigh Spellar
- Article Editor:
- Nagendra Gupta
- Updated:
- 8/8/2020 9:01:57 PM
- For CME on this topic:
- Diaphragmatic Hernia CME
- PubMed Link:
- Diaphragmatic Hernia
Introduction
A diaphragmatic hernia (DH) is a protrusion of abdominal contents into the thoracic cavity as a result of a defect within the diaphragm. It is most common as a congenital phenomenon; however, there have also been cases where it can be acquired.[1] Reports place its incidence at approximately 0.8-5/10,000 births. Most commonly, acquired DH occurs following blunt or penetrating trauma which results in a rupture of the diaphragm which is then accompanied by herniation of abdominal content. Additionally, there are cases reported where acquired DH can also occur spontaneously or by iatrogenic causes.[2] Acquired DH is rare but can be life-threatening, resulting in incarceration and strangulation with an overall mortality rate up to 31%.[3]
Etiology
The most common etiology of acquired diaphragmatic hernia (ADH) is secondary to trauma which results in diaphragmatic rupture. It occurs more often from blunt trauma but can also result from penetrating thoracoabdominal trauma.[4] Diaphragmatic rupture from thoracoabdominal trauma occurs in approximately 0.8 to 3.6% of cases, with the incidence of herniation following such an event being relatively low.[4][5] Iatrogenic causes following surgery are the second most common cause of ADH, however, are very rare, with mostly just case studies in the literature. The most common surgeries with which DH has been associated and reported is following pediatric liver transplants and liver resection.[6][7] Other noted documented episodes of ADH post-surgery within case studies include Nissen fundoplication, left colectomy, adrenalectomy, laparoscopy-assisted total gastrectomy, nephrectomy and partial resection of the left lung using thoracoscopic surgery.[8][9][10][11][12][13][14] Spontaneous defects have also been noted to occur, in these cases, they may be asymptomatic for years before becoming symptomatic in the later stage where the defects can be extensive.[2] Other rare causes documented within case studies include following radio-frequency ablation for hepatocellular carcinoma and during pregnancy.[15][16][17]
Epidemiology
Acquired diaphragmatic hernia is rare. Diaphragmatic rupture from thoracoabdominal trauma occurs in approximately 0.8 to 3.6% of cases, with the incidence of herniation following this being relatively low.[4][5] The number of patients affected by ADH from other causes is not clearly documented and is most commonly noted within case studies.
Pathophysiology
Acquired diaphragmatic hernia (ADH) as a result of trauma to the diaphragm is likely to occur at areas of potential weakness along embryological points of fusion of the diaphragm.[18] It is thought to be produced by a sudden increase in the pleuroperitoneal pressure gradient as a result of the trauma.[18] Multiple factors may result from to iatrogenic causes depending on the type of surgery, patient-related factors, and technique used to close the diaphragm.[7] ADH and diaphragmatic rupture tend to occur more commonly on the left side of the diaphragm. This tendency is likely due to the right hemidiaphragm being protected by the size of the liver beneath it.[19] Right-sided ruptures and herniations are very rare and associated with higher mortality and morbidity rate.[18] The abdominal contents that can herniate into the diaphragm vary, but documented cases include herniation of stomach, small intestine, mesentery, splenic and pancreas.[3]
History and Physical
Most ADH cases follow episodes of trauma, either blunt or penetrating to the thorax or abdomen. A clear history of trauma should prompt appropriate imaging to determine the extent of the injury, which may then demonstrate the presence of ADH. For other causes of ADH, it is crucial to consider the patient's previous surgical history as this may provide a cause of the ADH. Patients can present with ADH in a variety of ways. AHD may produce respiratory, abdominal and in some cases cardiac symptoms.[20] The effect from the abdominal contents putting pressure on the thorax can result in shortness of breath and chest pain. Abdominal symptoms may also be present, including recurrent abdominal pain, postprandial fullness, vomiting, and obstructive gastrointestinal symptoms.[18] In some spontaneous cases, the DH may remain asymptomatic, only revealed upon imaging studies. Examination of the patient may reveal the absence of breath sounds over the lower chest area, with bowel sounds being audible.[21]
Evaluation
Imaging is vital for diagnosis of acquired diaphragmatic hernia. A variety of different imaging modalities are used to diagnose or aid diagnosis of a diaphragmatic hernia including chest radiographs, ultrasonography, and magnetic resonance imaging, with computed tomography (CT) being the modality of choice.[21]
Treatment / Management
Treatment of acquired diaphragmatic hernia in the acute setting requires appropriate resuscitation of the patient.[2] Management following this is surgical. Typically, the procedure will use an open abdominal approach, and the repair accomplished by primary closure.[14] In cases where primary closure with non-absorbable sutures is not possible because of the size of the defect then mesh repair may be an alternative.[18] If the diagnosis is delayed, then a thoracic approach is generally preferred to reduce viscera-pleural adhesions and intra-thoracic visceral perforation.[18] It may be appropriate in some delayed cases to use a combined thoracic-abdominal approach. A laparoscopic approach may be feasible and could be an option for repair-dependent upon experience.[14]
Differential Diagnosis
There is a broad range of differential diagnosis for ADH considering the variation in presentation and the variety of symptoms associated with it. Before imaging, a diaphragmatic hernia is unlikely to be high up the differential list for causation of the patient symptoms, except perhaps in cases associated with trauma. After imaging, an alternative diagnosis that should merit consideration is metastasis, particularly with small defects.[20] Congenital causes of a diaphragmatic hernia should always be a consideration particularly when trauma has not occurred previous to the presentation.[22]
Prognosis
If the clinician misses the diagnosis of acquired diaphragmatic hernia then there is a substantial risk of death; this can be due to lung compression with respiratory failure, vascular compromise with gastric or intestinal infarction, or perforation.[23] There is a documented variable risk in surgical mortality for diaphragmatic repair depending on concomitant injuries between 5 to 50%.[2] Generally, the outcomes following correction are good, with recurrence levels being low.[2]
Complications
Deterrence and Patient Education
Most cases of acquired diaphragmatic hernia occur in emergencies following trauma; in these situations, surgery is life-saving. If possible, consent for surgery should be obtained with an explanation of the potential complications from surgery. These should be balanced with the complications including death if the surgery is not carried out.
Enhancing Healthcare Team Outcomes
Acquired diaphragmatic hernia is a serious condition which requires urgent surgery in the majority of cases. Imaging is vital for diagnosis however may be difficult to interpret particularly with additional damage from trauma, discussion between radiologist and surgeons is essential to enhance decisions in treatment. There is no consistent and recommended approach to surgery, with a variety of different methods and options being available. Typically, the repair will be carried out by general surgeons. However, if there is a delay in diagnosis, a thoracic approach may be required, and communication with the cardiothoracic surgeons can be crucial. Acquired diaphragmatic hernia is rare, so information regarding treatment meaning case studies may be vital in aiding with complicated cases in determining surgical approach (level 5).
(Click Image to Enlarge)
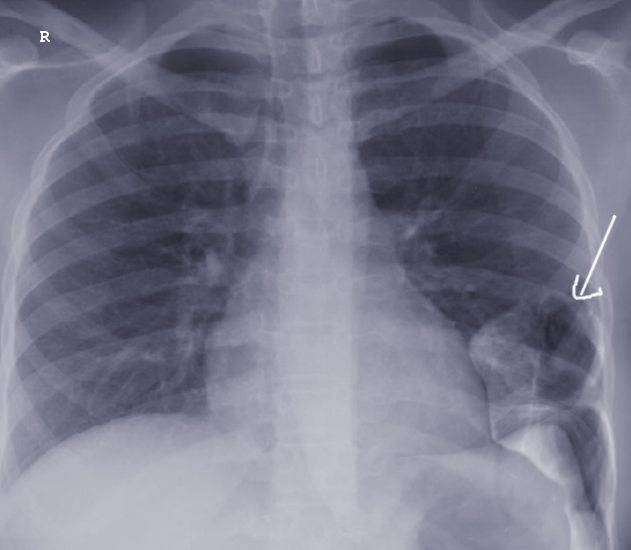
Acquired Diaphragmatic Hernia
Image courtesy S Bhimji MD
(Click Image to Enlarge)

delayed diaphragmatic hernia on CT imaging
Contributed by Mark Pellegrini (Public Domain)