Egophony
- Article Author:
- Pranav Modi
- Article Editor:
- Tripti Nagdev
- Updated:
- 7/10/2020 11:00:07 AM
- For CME on this topic:
- Egophony CME
- PubMed Link:
- Egophony
Introduction
In the era of technological advances, a thorough examination of the respiratory system retains its importance in diagnosing disorders of the respiratory system. Auscultation of the chest is among the oldest bedside diagnostic techniques used to assess airflow through airways. It is an easy, safe, non-invasive and cost-effective diagnostic technique. [1] The majority of the manifestations of respiratory disease present with abnormalities of chest examination. Egophony is increased resonance of voice sounds heard when auscultating the lungs. When spoken voices are auscultated over the chest, a nasal quality is imparted to the sound which resembles the bleating of a goat. Egophony (also known as “E” to “A” change) is an auscultatory finding due to a change in the quality (timbre) of the voice. A solid (consolidated), fluid-filled, or compressed lung decreases the amplitude and only allows select frequencies to pass through. This changes the sound of the vowel “E” to "A." [2]
Pathophysiology
Over the years there have been various theories explaining the mechanism of egophony. In 1894, Dr. Frederick Taylor described egophony as a musical discord. [3] Transmission of sound vibrations from the larynx and tracheobronchial tree to the chest wall depends on the state of the underlying lung tissue and surrounding pleural space. In the lung of a typical individual, air-filled spaces are surrounded by solid parenchymal tissue. Egophony is commonly seen in pneumonia (consolidation) and pleural effusion.
Mechanism of egophony in consolidation
The sound of the vowel "E" has a low frequency in the range of 100 to 200 Hz as compared to the low frequency of "A" which may reach up to 600 Hz. The sound "E" consists of a high frequency in the range of 2000 to 3500 Hz. Consolidation creates a dense medium that facilitates the transmission of lower frequencies. Hence in a patient with an underlying consolidation, an "E" is transformed into an "A." [1]
Mechanism of egophony in pleural effusion
In the case of pleural effusion, fluid accumulates in the pleural space. This fluid compresses the overlying lung parenchyma, making it more solid than usual. Due to this change, there is an alteration in the lung acoustics that preferentially transmits higher sound frequencies and gives rise to an egophony. [1] Egophony in pleural effusion is characteristically heard at the upper border of the effusion.
Technique
Examination Method
Inspection, percussion, palpation, and auscultation are essential components of the chest examination. Adventitious sounds provide clues regarding the underlying respiratory disease. The patient should be auscultated in a quiet room with the chest piece of the stethoscope in direct contact with the skin; it is preferable to have the patient remove clothing. The anterior and posterior chest walls along with the axillary region are commonly auscultated. Assess for symmetry, quality, and intensity of breath sounds.
Normal or vesicular breath sound is a low pitched, soft sound with a rustling quality. It is characterized by a prolonged inspiratory and short and soft expiratory phase. Vesicular sounds are produced due to turbulent air flow through the alveoli, lobar and segmental airways (inspiratory phase), and central airways (expiratory phase). On the other hand, bronchial breath sounds are loud, hollow, and high pitched sounds that are normally heard over the sternal manubrium and posterior chest wall due to movement of air through the trachea and large airways. Bronchial breath sounds heard in other areas could be due to any of the following underlying pathologies:
- Consolidation (e.g., pneumonia)
- Pleural effusion (bronchial breath sound can be auscultated above the level of the effusion)
- Pulmonary fibrosis
- Atelectasis
- Tension pneumothorax
- Lung mass over a patent bronchus
Voice sounds
Voice sounds are produced when air passes through vocal cords making them vibrate. In a healthy individual, these sounds are not audible. However, when consolidation or fluid replaces the air in the lung parenchyma, these sounds are better transmitted. Egophony is one type of a voice sound. The word "egophony" is derived from the Greek word "ego" which means "goat."
During auscultation, the patient is asked to say “Eee.” The “Eee” will be transformed into an “A” with the voice having a nasal or bleating quality (like the bleating of a goat). Egophony is seen in cases of consolidation, pleural effusion, and lung cavity.
Other voice sounds
- Bronchophony: While auscultating the lung fields, the patient is asked to repeat "99." Bronchophony is present if the "99" appears louder and more distinct over certain areas, suggesting underlying consolidation.
- Whispering pectoriloquy: The patient is asked to whisper "1-2-3" or "99." Whispering pectoriloquy is present if the whisper is heard more clearly over certain areas, suggesting underlying consolidation. [1]
Clinical Significance
Usefulness of Egophony in Daily Clinical Practice
A study among 52 men with symptoms of lower respiratory tract infection presenting in the emergency department of a Veterans Affairs medical center was conducted to determine the reliability of chest examination and assess the degree of agreement between three examiners. Twenty-four were diagnosed with pneumonia on X-ray. The results showed auscultatory percussion, egophony, and rales were among the most helpful maneuvers with the highest specificity. [4]
On the other hand, a literature review of 40 publications on the reliability and validity of respiratory physical examination showed low-to-fair inter-examiner agreement rates for egophony and other signs like bronchophony, pectoriloquy, vocal resonance, and pleural friction rub. To assess the pre-test probability of a condition like pneumonia, it is not certain if using a combination of physical signs (consolidation: dull to percuss, egophony, bronchophony) increases the likelihood ratio (multiplication of each of their likelihood ratios). [5]
Important Clinical Findings in Pneumonia
On inspection, diminished chest movements may be seen on the affected side. A vocal fremitus may be palpated along with a dull note on percussion on the affected side. Bronchial breathing sounds may be present on auscultation. Vocal resonance is increased on the affected side which may be associated with bronchophony, egophony, and whispering pectoriloquy. [6]
Important Clinical Findings in Pleural Effusion
On inspection, a fullness of intercostal spaces with diminished chest movements on the affected side may be seen. On palpation, vocal fremitus is decreased on the affected side. The trachea may be shifted to the opposite side in the presence of a large effusion, and the apical impulse may not be palpable. A stony dullness is usually present on percussion of the affected side. As explained, an egophony can be auscultated on the upper border of the effusion with diminished breath sounds and vocal resonance on the affected side. [6]
Enhancing Healthcare Team Outcomes
Healthcare workers including nurses who look after medical and surgical patients should know how to use a stethoscope. While not a replacement for imaging studies, this technique can help detect several thoracic pathologies at the bed side. This can be time saving and saves sending an ill patient to an unmonitored radiology suite.
(Click Image to Enlarge)
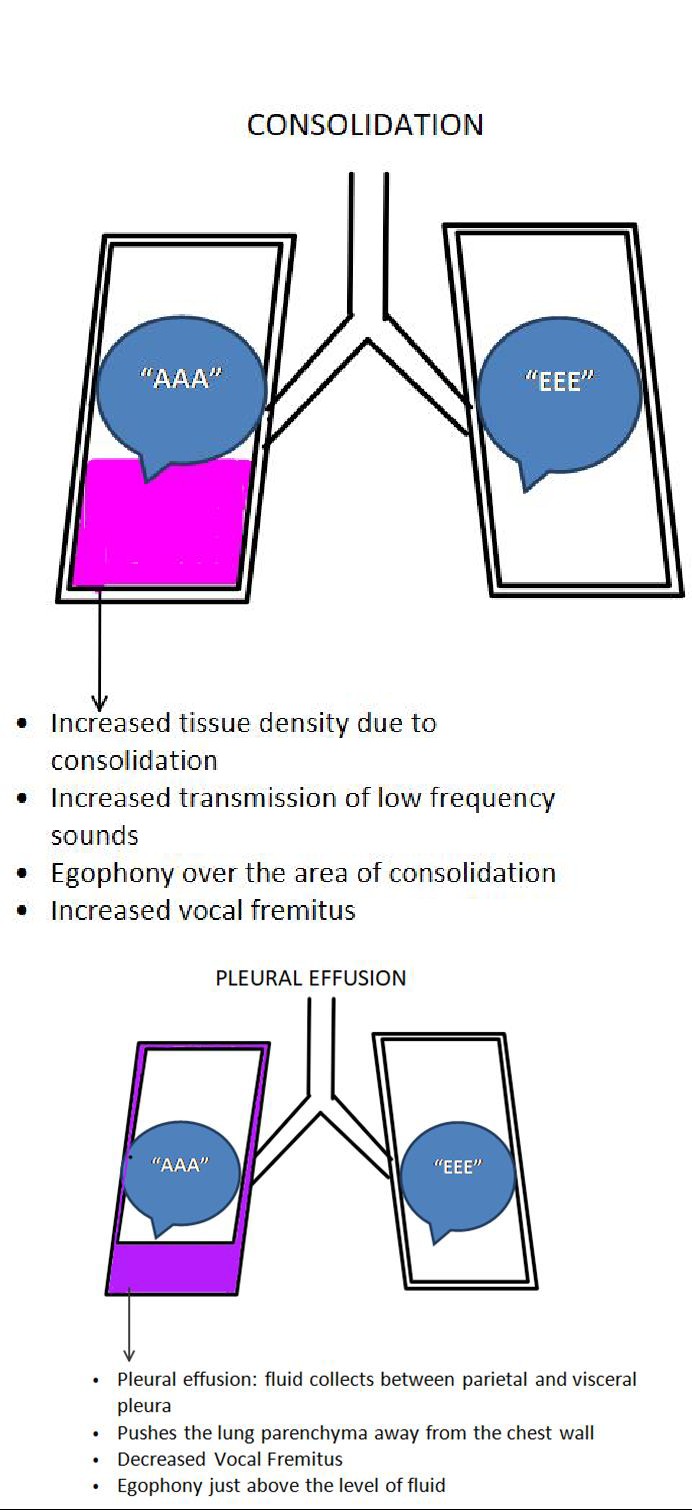
Consolidation and Plueral Effusion
Contributed by Pranav Modi