Platysmaplasty Facelift
- Article Author:
- Leon Alexander
- Article Editor:
- Bhupendra Patel
- Updated:
- 9/22/2020 11:50:01 AM
- For CME on this topic:
- Platysmaplasty Facelift CME
- PubMed Link:
- Platysmaplasty Facelift
Introduction
Platysmaplasty is a rejuvenation procedure performed to increase the definition of the neck from the angle of the jaw to the chin, thereby restoring a youthful and aesthetic contour to the face. It is generally indicated in persons between 40 to 60 years of age and for those who want jaw-neck definition. It is not suitable for patients above 60 years age who have lots of excess skin and fat in the neck. For these patients, other procedures like a full or short scar facelift and liposuction have to be added along with a plastymaplasty. However, platysmaplasty is most commonly performed in conjunction with a full cervicofacial rhytidectomy where the aim is to improve everything below the lower eyelids and up to the clavicles.[1]
Bourguet (1928) was the first to describe a variation of the modern-day platysmaplasty, where he used a sub-mental incision to divide the prominent platysma muscle. Skoog (1969) presented a one-layer neck lift in which skin, subcutaneous and platysma muscle was suspended up through a lateral facelift incision. Guerro–Santos (1978) first described lateral imbrication of the platysma to the fascia of the sternocleidomastoid and mastoid. Feldman (1988) pioneered the technique of corset platysmaplasty wherein the two halves of muscle were sutured together and further cinched and shaped to recreate the youthful aesthetic neckline. Fuente del Campo (1998) published the “hammock platysmaplasty” technique, in which a double-breasting type of plication of the platysma to the contralateral mastoid fascia was performed.[2][3][4][5]
There have been many other variations to these initial techniques which involve the use of fascia, meshes, small-incision insertion of supporting sutures, and small-incision platysmal plication with subcutaneous treatment with plasma to create skin contraction.[6]
Anatomy and Physiology
The neck is a complex anatomical structure. To obtain a youthful and aesthetically pleasing contour, a thorough knowledge of its anatomy and physiology is mandatory for the operating surgeon.
The neck is divided into three aesthetic subunits, (1) chin subunit, (2) submental subunit, and (3) anterior neck subunit. Anatomically, the neck has three layers; skin, superficial fascial, and deep fascia. The superficial fascia consists of fat, connective tissue, platysma muscle, superficial veins, lymph nodes, and cutaneous nerves. The deep fascia has three layers – The external or investing layer of deep fascia, middle or pretracheal fascia, and the deep or inner prevertebral fascia.
The platysma is a broad, slim muscle located in the anterolateral aspect of the neck, thicker in men than in women (Fig). It is supplied by the cervical branch of the facial nerve, which travels beneath the muscle, and its action is to assist in depressing the lower lip in concert with the depressor anguli oris. The platysma is a continuation of the superficial musculoaponeurotic system (SMAS) just below the inferior border of the mandible. Both the SMAS and platysma divide the subcutaneous fat of the neck and face into two layers. The subplatysmal plane in the neck contains the deep layer of fat, facial nerve branches, submandibular gland, the tail of parotid, and the external jugular vein. In the submental and suprahyoid region, a thick fat layer overlies the platysma, which becomes thinner inferiorly, such that the platysma lies in close approximation to the skin.
It is essential to know the anatomy of the marginal mandibular, the cervical branches of the facial nerve, and the great auricular nerve (GAN) when performing a neck lift or a cervicofacial rhytidectomy.
The marginal mandibular nerve exits from the anteroinferior portion of the parotid gland and courses anteriorly and deep to the SMAS and platysma. It then courses along the inferior border of the mandible. At the mid-body of the mandible, it becomes superficial between the platysma and deep fascia, crosses the anterior facial artery to supply the depressor labii inferioris and mentalis muscle. The ‘danger area’ of the marginal mandibular nerve extends from the angle of the mandible to the anterior facial artery where it is most prone to injury if the dissection goes deep to platysma in this region. Therefore, the safe plane of dissection here is superficial to the platysma.
The cervical branch of the facial nerve, which supplies the platysma, travels along with the marginal mandibular nerve (20%), or after exiting the parotid gland, it travels posterior to the angle of the mandible (80%). Ultimately, both branches diverge at the submandibular gland just anterior to the hyoid bone. The ‘danger area” for the cervical branch is at the level of the hyoid bone when the dissection is deep to the platysma. Therefore, when performing a neck lift, the surgeon must be extra-cautious while dissecting deep to the platysma in the posterior neck.
The most commonly injured nerve in rhytidectomy is the great auricular nerve (GAN). It emerges from the posterior border of the sternocleidomastoid muscle at a point 6.5cm inferior to the external auditory meatus. It is a sensory nerve and supplies the cutaneous territory over the parotid gland and lobule of the ear. During posterior skin flap elevation, the surgeon must be careful to avoid elevating a thick flap that runs deep into the subcutaneous layer, as the GAN runs very superficial in this area.
An attractive youthful neck is defined by the following criteria which are used in the evaluation of age-related changes in the neck, including:[7]
- Cervico-mental angle (CMA) is the angle between the chin and the neck. It should be well defined, with the ideal being between 105 and 120 degrees.
- Mental prominence – The mentum or chin should be prominent, well defined, and sculpted on anterior and profile views.
- Hyoid Position – The ideal position of the hyoid bone is superior and posterior in relation to the CMA, thereby creating an acute and prominent CMA.
- Well defined inferior mandibular border
- Visible anterior border of the sternocleidomastoid (SCM)
- Subhyoid depression
- Visible thyroid bulge (thyroid cartilage)
Some of the age-related changes leading to neck deformities can be attributed to a loss of skin elasticity due to degeneration of dermal collagen and elastin, accumulation of fat, years of sun damage, lipodystrophy, and hormonal changes. With aging, the platysma muscle becomes lax, and the fascia supporting the midline decussation also attenuates, leading to a hanging medial border of platysma forming the platysma bands. The lateral border of muscle also sags, leading to bands. Additionally, there is ptosis of submandibular glands leading to loss of definition of the mandibular border. There is also attenuation and relaxation of retaining ligaments of the face and neck. The zygomatic and masseteric cutaneous ligaments become lax and stretch, leading to a descent of facial soft tissue below onto the neck and lead to prominent nasolabial fold and distortion of neck-face definition. Similarly, labiomandibular folds (jowls) are caused by weakening and stretching of the masseteric cutaneous ligament (MCL) and mandibulocutaneous (mandibular) ligaments, which allow the excess and lax soft tissue of the cheek to descend and spill over the inferior border of mandible forming jowls. Fat accumulation is seen within jowls.[1]
The secondary changes which contribute to the aged neck include prominent labiomandibular folds or jowls, prominent nasolabial folds associated with facial soft tissue descent, loss of volume of the bony facial skeleton, and submental fullness. However, recent studies have challenged the concept that platysma bands are due to sagging skin and muscular atonia, and that they are actually caused by muscular hyperactivity.[8][9][10][11][12][13][14][15][16]
Indications
Platysmaplasty is an elective cosmetic procedure and is indicated in those patients who want to reverse the age-related changes in the neck, such as loose, saggy skin, platysma bands/cords (Turkey-gobbler neck), and excess fat in the neck. A standard facelift (cervicofacial rhytidectomy) will adequately address most of the age-related neck changes and remains the gold standard, but for those patients who are unwilling to undergo a facelift, the neck lift or platysmaplasty remains an acceptable compromise.
Giampapa and Di Bernardo have proposed the following five criteria for neck lift;
- A poorly defined CMA
- A poorly defined inferior mandibular border or jawline
- Absence of laxity in the midfacial structures
- Small to moderate amounts of jowl and neck fat
- Patients who do not want to undergo a full facelift
Certain absolute indications of midline platysmaplasty include,
- Patients with excessive redundancy in platysmal banding (depth more than 1.5cm) and not corrected by lateral suspension/advancement of platysma
- Subplatysmal lipectomy, if performed, must be combined with midline platysmaplasty.
- Patients with type III decussation pattern platysma (platysma muscle split apart or dehisced from midline).[17][18][17]
Contraindications
There are no absolute contraindications, but certain patients are not good candidates for surgery. These include:
- Patients with unrealistic expectations
- Patients with psychiatric problems (body dysmorphic disorder, psychosis, mania, and major depression)
- Heavy smokers who refuse to stop smoking at least one month before surgery
- Patients who are medically unfit for surgery
- Patients who are on certain drugs like isotretinoin, which may lead to poor wound healing.[19]
- Patients with significant changes along the jawline, jowls, and midfacial ptosis
Equipment
Equipment required for platysmaplasty includes standard fine plastic surgery instruments:
- Long and medium-length needle holder
- Webster needle holder
- Metzenbaum scissors with fine, curved, blunt tips (for undermining of platysma)
- Deaver retractor
- Lighted retractors
- Fine Mayo or McIndoe scissors
- Skin hooks
- Adson forceps
- Barron knife holder
- Fine bipolar handles
- Monopolar hand switch
- Liposuction cannulas
- Nerve hooks
- Tissue elevators or dissectors
- Headlight and loupes
Personnel
The personnel involved in this procedure should include surgeon, surgeon assistant, scrub nurse, anaesthetist, anaesthesia technician, circulating nurse and postoperative care nurse.
Preparation
Preparation before the surgery involves a detailed history, clinical examination, pre-operative photography, blood workup, and other investigations and an anesthetic assessment. Clinical assessment of the signs of facial aging must include the following:
- Amount of skin excess/laxity
- Thickness and elasticity of the skin
- Signs of photoaging and solar actinosis
- Assessment of rhytids at rest and on animation. Skin pinch tests should be performed to assess the quality, thickness, and amount of fat below the skin, also at rest and animation.
It is essential to assess for excess skin along with the sternocleidomastoid muscle and chin and thyroid cartilage area. The submental and neck fat must be evaluated, including the amount of subcutaneous and sub-platysmal fat; the two fat compartments can be differentiated by pinching the skin at rest and after the contraction of the platysmal muscle. When there is a reduced skin pinch size on animation, it signifies excess subplatysmal fat and vice versa. It is also vital to assess the amount of excess skin in the neck and platysma bands both at rest and on animation. The submandibular glands and digastric muscle should also be examined by looking for a bulge below the inferior mandibular border and even on neck flexion.
Patients are also advised to discontinue aspirin, non-steroidal anti-inflammatory drugs, herbal supplements, and other anticoagulants two weeks before surgery.
We mark the skin markings with the patient upright before surgery, using the patient's ability to smile, contract the platysma, and flexing of the neck to allow an accurate assessment and to mark the important structures. These include the marking of the submental incision line, jowl lines, mandibular borders, subcutaneous fat prominences in the neck, platysmal neck bands, anterior border of SCM, external jugular veins, and markings for the facelift are also done if it is planned concomitantly with plastymaplasty. The estimated site of the greater auricular nerve is also marked on the neck. After induction of general anesthesia, the patient is scrubbed and draped in a sterile fashion. Tumescent local anesthetic solution (0.1% lidocaine with 1 in 1,000,000 adrenaline) is injected into the skin markings, and the subcutaneous neck is infiltrated with at least 100 ml of this solution.
Technique
Over the last 50 years, many different techniques of neck lift/platysmaplasty have been described for the rejuvenation of the aging neck. Platysmaplasty is usually combined with submental liposuction and a full facelift as indicated. Other ancillary procedures performed along with platysmaplasty when indicated include supraplatysmal fat reduction, subplatysmal lipectomy, submandibular gland reduction, and partial digastric myectomy. A wide array of platysmaplasties have been described in the literature, such as the midline platysmaplasty, corset platysmaplasty, different suture techniques (plication, imbrication, overlap, suture suspension, sling platysmaplasty, and pursestring sutures), lateral platysmapexy, transverse platysma myotomy, and partial platysma myectomy.[1]
Anterior (medial) Platysmaplasty
This is the most commonly performed technique and entails midline approximation of the platysmal diastasis from the chin to the thyroid cartilage. A transverse skin crease incision is made just caudal to the submental fold, and the skin is undermined caudally to the cricoid cartilage and beyond. Next, the platysmal bands are corrected by separating the muscle in the midline and from the anterior belly of digastrics.
Before approximation, the redundant medial muscle borders are trimmed and sutured together without invagination or imbrication in a smooth edge-edge fashion (FIg). At this stage, depending on the patient, a decision is made intraoperatively whether to excise the subplatysmal fat. This procedure is not adequate to treat excess subplatysmal fat, prominent submandibular glands, or anterior belly of the digastric muscle and 'hard', dynamic platysmal bands. When concomitant facelift and neck lift is done, platysmaplasty should be performed after cheek-SMAS flap dissection and suspension as it provides optimal correction of cheek folds and jowls and the best longterm result.
Lateral platysmapexy/platysmaplasty
Lateral platysmapexy is performed when there is a mild horizontal redundancy of platysma and can be performed when a neck lift is combined with a facelift. This procedure is usually performed after medial platysmaplasty and involves the suturing of platysma to the upper one-fourth of SCM fascia. Some authors advocate anchoring the lateral border of the platysma to the preauricular platysma auricular fascia (PAF) giving a more vertical vector to the support and lift. This ensures an even smooth neck contour and consolidates a neck lift further.
When a horizontal platysmal redundancy is excessive, then a postauricular transposition flap (PATF) of cheek SMAS-platysma is planned. The PATF is then sutured to the mastoid fascia on both sides, and this leads to an optimal reduction of horizontal platysma redundancy and also an effective reinforcement when the patient looks down. This procedure is usually combined with a facelift and should be performed only after anterior/medial platysmaplasty has been completed.
Corset Platysmaplasty (Feldman)
This is a type of anterior platysmaplasty where the medial borders of platysma after trimming are sutured with a continuous monofilament suture that is run up and down the midline neck until the desired result is obtained (Fig). Some authors prefer buried interrupted sutures and may do this conjunction with a full facelift and lateral platysmapexy depending on the indication. Performing just a corset platysmaplasty without lateral and superior support is now thought to run the risk of bringing the platysma downwards, possibly resulting in failure of the procedure.
Hammock Platysmaplasty (Platysmal Overlap)
Fuente del Campo first described this technique of platysma overlap in the midline; he called it hammock platysmaplasty. It consists of overlapping the platysma in a double-breasted fashion in the middle of the neck and gives good functional muscular reconstruction and cosmesis. It was subsequently modified by Gentile, in which he used interlacing sutures through the platysma, resulting in a medial to lateral plication.
Pursestring Platysmaplasty
This technique involves interlacing a suture through the platysma in a circular fashion When the suture is tightened, the platysma inverts and folds thereby reducing its surface area leading to a deepening of the fold just below the mandibular border and creating a well-defined mandibular border. Three varieties of pursestring platysmaplasty have been described:
Type I Pursestring platysmaplasty simply involves placing interlacing sutures just below the angle of the mandible and following its border to define it further.
Type II Pursestring platysmaplasty involves overlapping sutures on the medial border of platysma simulating a Hammock platysmaplasty.
Type III Pursestring platysmaplasty – in this type continuous interlacing sutures are placed starting from the mastoid fascia on one side to the contralateral side and back again. Initially, non-absorbable sutures were used, but now expanded polytetrafluoroethylene (ePTFE) and barbed sutures (polypropylene Quill) are used.
Suture Sling Platysmaplasty
In this technique, after plication and suspension of the SMAS-Platysma complex, a suture or broader structure (ePTFE implant) may be used to offer additional intrinsic and extrinsic support. Conrad was the first to describe using an ePTFE implant which is used as a sling to support the submental structures leading to a sharper, more defined CMA. This evolving cervical sling technique gives excellent and predictable results for the correction of obtuse CMA; an added advantage is that secondary adjustments are possible for rebound laxity of neck tissue and submental redundancy.
Recent advances include the use of absorbable bioimplants like polymeric ribbon suspension device made of polylactic acid and polyglycolic acid (PLA/PGA), which are inserted using minimal incisions and used to redrape the platysma to improve neck contour.
Transverse Platysma Myotomy
This technique is indicated to remove dynamic platysmal banding or striations that appear during conversation and on animation. Platysma myotomy must be performed only after anterior platysmaplasty and lateral platysmapexy have been completed to ensure a uniform redraping and distribution of platysma around the neck and a resulting smooth contour. Platysma myotomy is usually performed low in the neck at the level of cricoid cartilage as at this level the muscle is thin and is less likely to bleed. Furthermore, a smooth transition to CMA is obtained, and more importantly, lower lip complications are avoided.
Partial Platysma Myectomy
Partial Platysma Myectomy involves the excision of a part of the platysma muscle with a full-width transection at a high mid-thyroid cartilage level. This procedure is the most effective way to recreate the smooth contour in difficult necks of patients who have undergone multiple previous invasive and non-invasive skin tightening procedures and present with secondary irregularities, dense subcutaneous fibrosis, muscle fibrosis leading to both resting and dynamic platysmal bands, and an elderly 'skin on muscle' appearance. Such patients are refractory to the traditional platysmaplasties and will require partial platysma myectomy and later a secondary fat grafting.
An important point to note is that when performing a partial platysma myectomy one must maintain a cuff of muscle posteriorly at the CMA to avoid injuring the marginal mandibular and cervical branches of the facial nerve.
Final Closure and Assessment
Once the neck lift and/or facelift has been completed, the final contouring of the superficial cervicofacial fat is performed. It is usually done under direct vision using the scissors technique. Still, it is vital to avoid over resection of fat as it can lead to a skeletonization of the neck and an unnatural result. This final fat sculpting ensures an even, smooth contour to the neck and a predictable outcome. This is followed by drain placement which is routinely done in all primary and secondary neck lifts to avoid troublesome postoperative hematomas and seromas. After the final confirmation of adequate hemostasis and neck contour, the submental incision is closed in two layers.
The patient's hair is washed and shampooed in the recovery room, allowed to dry and tied, a final inspection is made of all the suture sites and drains. Typically no dressing is required, and patients are discharged the same day, prescribed oral antibiotics and analgesics for a week, advised to avoid direct sunlight for a few days, to sleep in an elevated head-up position, and to review if there is any bleeding, hematoma or infection in the wound.[20][21][18][22][23][24][25][26][27][28]
Complications
Complications following plastysmaplasty can be divided into early and late complications.
Early complications include hematoma, seroma, wound infection, marginal mandibular nerve injury/neuropraxia, cervical branch neuropraxia, great auricular nerve (GAN) injury, wound infection, sialoma, and salivary fistulas.
Late complications include contour irregularities, asymmetrical fat removal, inadequate reduction, overcorrection, visible platysmal banding, and neck overskeletalization.
Management of Complications
Small hematomas can be drained percutaneously in the clinic. Still, significant expanding hematomas are a surgical emergency as they may cause airway compromise and skin flap necrosis. Hence the need to be expeditiously drained in the operating room followed by the insertion of a continuous suction drain.
Marginal mandibular nerve injury or neuropraxia is the most commonly injured motor nerve and results in weakness of the ipsilateral lower lip due to denervation of the depressor anguli oris, depressor labii inferioris, and mentalis muscles. Re-exploration for marginal mandibular nerve injury is generally not indicated as most of these are traction injuries and resolve with time and simply require regular follow up and reassurance. However, marginal mandibular nerve injuries are more likely to be permanent if severe because of the unusual anatomy. The use of botulinum toxin to weaken the contralateral hyperactive lower lip muscles is a useful temporary measure till the neuropraxia resolves.
Injury to the cervical branch of the facial nerve gives rise to a pseudoparalysis mimicking marginal mandibular nerve injury as the platysma assists in the depression of the corner of the mouth and can also affect the ability of the patient to smile. These injuries are differentiated from the marginal mandibular nerve injuries as the patient will be able to evert the lip in pseudoparalysis because of an intact mentalis muscle. Full recovery is the rule in the majority of these cases.
Great auricular nerve (GAN) injury is the most commonly injured nerve in a neck lift. Injuries to the GAN present as numbness around the pre-auricular region and ear lobe, sometimes it can also lead to a painful neuroma and mass formation. Surgical exploration and excision of neuroma are indicated in such cases.
Persistent platysma bands can be treated non-surgically by the use of botulinum toxin or re-excision and redraping of the neck skin. Contour irregularities can be corrected by fat grafting and redraping of skin.[14][16][20][29][30][31][32]
Clinical Significance
Platymaplasty is one of the neck rejuvenation techniques used in patients who want to improve the appearance of their necks by improving unwanted platysmal bands, jowls, and neck fat. This procedure is primarily indicated in patients who are in the age range from 40 to 60 years and do not want a full facelift surgery but just want an aesthetic and pleasing neck with a smooth contour and well-defined borders. This procedure can be combined with other ancillary techniques like submental liposuction, sub-platysmal fat excision, submandibular gland, and digastric muscle excision to add more longevity and predictability to the final result.
Enhancing Healthcare Team Outcomes
With the increasing demand for rejuvenation procedures for the face and neck, neck lifts are in demand as many patients perceive them to be less invasive and scarring than facelifts, but it is essential that when treating such patients, a multidisciplinary team (MDT) approach is followed in order to avoid troublesome postoperative complications and litigation. The MDT for a neck lift patient should include a plastic surgeon as the captain of the ship and is assisted by other specialists, which include an internal medicine physician, anesthetist, psychiatrist, financial counselor, nurse-physician, pharmacist, and dermatologist.
Each member of this team has a specific and important role to play to deliver holistic care to the patient and to ensure that the process is smooth without any undue complications. For example, patients with psychiatric problems are not absolute contraindications for surgery, and if they are willing to acknowledge the limitations of surgery, do not have unrealistic expectations, take appropriate medications and undergo pre-operative and postoperative counseling, then in such situations, surgery can be undertaken without any untoward incident.
Another important factor in contributing to better outcomes is that though the complications following platysmaplasty are low, provided they are done by fellowship-trained and experienced plastic surgeons when they occur. It is a timely intervention that can make a difference. In this situation, an interprofessional team approach or MDT approach whereby physician nurses, specialized nurses, therapists, pharmacists, and ultimately the surgeon all play a vital role in ensuring the best and most predictable outcomes.
(Click Image to Enlarge)

Result of a deep-plane facelift. Note the re-volumization of the midface with improvement in the projection of the malar eminence, improvement of the jowl with appropriate platysmal and SMAS repositioning and buccal fat pad reduction.
Contributed by Prof. Bhupendra C. K. Patel MD, FRCS
(Click Image to Enlarge)

The platysma muscle: note the central separation of muscle fibers which occurs with age. The separation results in platysmal bands in the neck
Contributed by Professor Bhupendra C. K. Patel MD, FRCS
(Click Image to Enlarge)
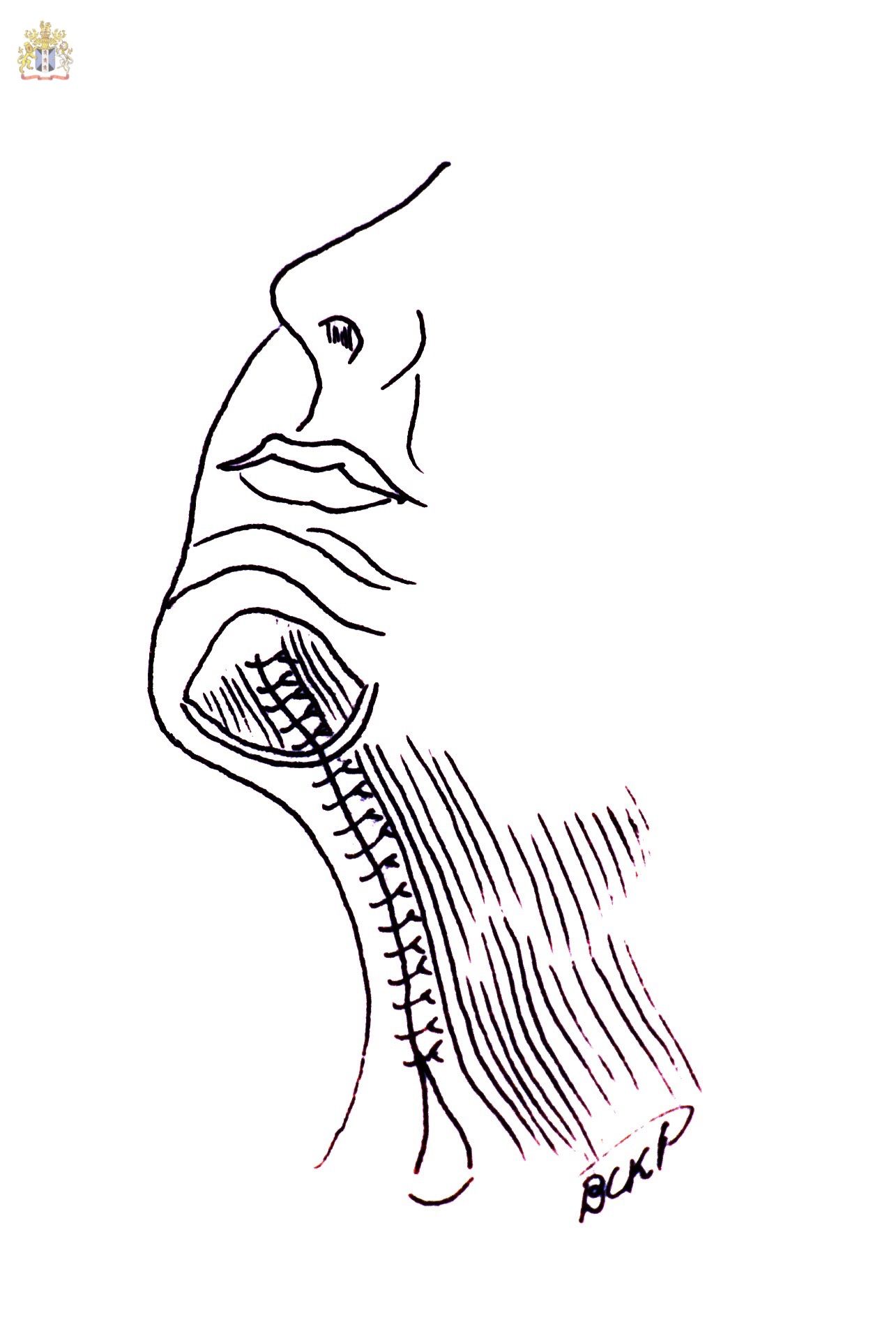
The Corset Platysmaplasty where the medial separated platysmal bands are sutured with two or three layers of sutures from the mentum to the supraclavicular zone. Some surgeons now feel that this may bring the platysma down and result in recurrence of bands in the neck and that a better way to manage the platysma is to tighten and lift it laterally and mostly superiorly with or without platysma myotomies.
Contributed by Professor Bhupendra C. K. Patel MD, FRCS