Felty Syndrome
- Article Author:
- Rosemina Patel
- Article Editor:
- Hossein Akhondi
- Updated:
- 7/6/2020 4:51:27 PM
- For CME on this topic:
- Felty Syndrome CME
- PubMed Link:
- Felty Syndrome
Introduction
Felty syndrome (FS) is an uncommon extra-articular manifestation of seropositive rheumatoid arthritis (RA) characterized by RA, neutropenia, and splenomegaly. Felty syndrome was first described in 1924 at Johns Hopkins hospital by the American physician, Augustus Felty. He described five unusual cases with common features of chronic arthritis of about four years duration, splenomegaly, and striking leukopenia. The term was first used by Hanrahan and Miller in 1932 when they described the beneficial effect of splenectomy in a patient with features similar to the five cases reported by Felty. While Felty syndrome characteristically demonstrates chronic arthritis, splenomegaly, and neutropenia; completion of the triad is not necessary for the diagnosis. Neutropenia, however, is a hallmark feature of the disease and cannot be absent.[1]
Etiology
There is strong evidence suggesting the presence of HLA-DRB1 allele shared epitope as a risk factor for anti-cyclic citrullinated peptide (CCP) antibody development. Rheumatoid factor (RF) and anti-CCP positivity are associated with an increased risk of development of extraarticular RA (ExRA).[2] HLA-DRB1 includes DRB1*01 and DRB1*04. HLADRB1*04 homozygosity has correlations with the development of more severe and erosive RA. A large multicenter study evaluating the impact of HLA-DRB1 genes in patients with ExRA confirmed a strong association of HLA-DRB1*0401 and FS. In the same study, there was a lack of association between ExRA and HLA-DQB1 alleles and DRB1-DQB1 haplotypes favoring the specific role of HLA-DRB1 genes.[3]
Epidemiology
Prevalence of Felty syndrome in patients with rheumatoid arthritis is reported to be around 1% to 3%.[4] With the evolution of RA pharmacotherapy, including increased use of methotrexate and biologics, the risk of Felty syndrome seems to be declining, and true prevalence is very low.[5] Felty syndrome usually develops about 16.1 years after RA presentation, with increased risk in patients with a positive family history of RA. There is also a stronger association of RA with HLA DR4 in patients with Felty syndrome.[1] The disease follows the same pattern as RA and affects females three times more than males, diagnosed in middle age, and affects the caucasian population more compared to African Americans.[6][7]
Pathophysiology
The exact pathophysiology of Felty syndrome is not clear, and it may be multifactorial. It is thought to involve both humoral and cellular immune mechanisms, which contribute to survival and proliferation defects of neutrophils resulting in neutropenia.[8] Neutropenia can be explained by inadequate production due to infiltration of bone marrow by cytotoxic lymphocytes and increased sequestration due to splenomegaly supported by the improvement of neutropenia after splenectomy. A case-control study done for the presence of antibodies against granulocyte-colony stimulating factor (G-CSF), showed that 73% of patients with neutropenia due to FS had IgG Anti-G-CSF, which was associated with an exaggerated serum level of G-CSF and a low neutrophil count. This finding suggests that a high level of G-CSF and hyposensitivity of myeloid cells to G-CSF might be responsible for the development of neutropenia in patients with Felty syndrome.[9] Another study concluded that autoantibodies present in FS bind to deaminated histones and neutrophil extracellular chromatin traps (NETs) leading to neutrophil sequestration, supporting the role of peripheral destruction of neutrophils in the pathophysiology of Felty syndrome.[10] Some have suggested that chronic large granular lymphocyte (LGL) leukemia and FS may have a common pathologic link because of similar clinical presentation and common genetic etiology of HLA-DR4.[11] Neutropenia in LGL leukemia has been attributed to increased secretion of circulating Fas ligand which induces neutrophil apoptosis. Patients with LGL leukemia also often have other autoimmune diseases like RA as well as elevated levels of Fas ligand, suggesting a similar pathogenic mechanism.[12][13]
History and Physical
Described as a manifestation of severe RA; Felty syndrome usually occurs in patients with severe, long-standing, erosive, and seropositive arthritis. However, the diagnosis of Felty syndrome can precede arthritis symptoms in a few cases.[14] Although articular involvement at the onset of FS can be quiet or active, most patients have radiographic evidence of erosive disease. Synovial effusions may be present in about 75% of patients.
Patients usually present with an infection because Felty syndrome is otherwise asymptomatic. The most common type of infection is dermatological and respiratory. Many patients have other extra-articular manifestations. These have been reported as rheumatoid nodules (74%), hepatomegaly (68%), lymphadenopathy (42%), Sjogren syndrome (48%), pulmonary fibrosis (50%), pleuritis (22%), peripheral neuropathy (14%), leg ulcers (16%). Systemic symptoms, including fever and weight loss, may also be present.[15] Although splenomegaly is present in most cases, the involvement of spleen is not necessary for diagnosis. Spleen is usually palpable on clinical examination. Some patients can also have idiopathic non-cirrhotic portal hypertension which can lead to variceal bleeding.
Evaluation
Complete Blood Count
Complete blood count with differential shows an absolute neutrophil count of less than 2000/microliter, which is a hallmark feature and required for the diagnosis of Felty syndrome, accounting for an increased risk of bacterial infections. Diagnosis of Felty syndrome can sometimes be made earlier if the patient’s blood counts are under surveillance for another reason, such as medications' toxicity monitoring. There is no correlation between splenic enlargement and degree of neutropenia.[16] Anemia and thrombocytopenia may be present in patients with splenic enlargement. Anemia of chronic inflammation is present in almost all patients.
Serology
Laboratory findings of RA, like positive rheumatoid factor (RF) and anti-CCP, are almost always present in FS. Antinuclear antibodies, anti-histone antibodies, and HLA-DR4 can also be present.
Imaging
Plain radiographs of small peripheral joints may show severe joint destruction. Imaging of spleen with ultrasound or radionuclide scan can be done to detect splenomegaly.
Bone Marrow Biopsy
Bone marrow biopsy shows myeloid hyperplasia in most cases with increased granulopoiesis and relative excess of immature forms described as “maturation arrest.”[15] Bone marrow biopsy helps rule out LGL leukemia, and a hypoplastic marrow should raise suspicion for other pathology. Immunophenotyping of marrow can also help to diagnose LGL leukemia.
Histology
Splenic histology in autopsies and post-splenectomy cases has shown non-specific findings such as congestion of venous sinusoids, reticular cell hyperplasia, and germinal cell hyperplasia.
Treatment / Management
Treatment for Felty syndrome focuses on controlling the underlying RA and treating the neutropenia to prevent infections.
The goal is to achieve a granulocyte count of more than 2000/microliter. Neutropenia without evidence of infection is not an indication for treatment; however, the presence of neutropenia in patients with RA can help in adjusting disease-modifying antirheumatic drugs (DMARD) therapy. Improvement of the neutrophil count with the treatment of RA indicates a component of FS. Patients with neutropenia should undergo a thorough examination to look for signs of infection. The presence of systemic symptoms should prompt treatment. Care of neutropenic patients involves good dental and oral hygiene as well as scheduled age-appropriate immunizations. The clinician should initiate appropriate treatment of infections with broad-spectrum antibiotics, and neutropenic precautions are necessary. An infectious disease specialist consult can be helpful.
There are no randomized control studies available for the treatment of Felty syndrome, and most of the data directing treatment are from observational studies. Low dose oral methotrexate is considered first-line treatment. It has demonstrated benefit in the improvement of neutrophil count and helpful in preventing recurrence of infection. Studies have shown that a dose of less than 7.5mg/week results in prompt improvement of neutrophil count within 4 to 6 weeks. Because the effect of methotrexate is dose-dependent with noticeable change seen after 4 to 8 weeks, an adequate trial with a maximum tolerated dose should be considered before deeming it unresponsive.[17][18][19]
Other DMARDs have been reported to be beneficial in some reports. A case report described a patient with RA who developed Felty syndrome while on MTX therapy and then severe cutaneous allergy to etanercept, but subsequently, significant improvement in neutropenia with leflunomide.[20] Parenteral gold therapy was previously used in Felty syndrome but is outdated now due to the extensive adverse side effect profile.[21] Cyclosporine has shown response in a few reports but is not generally an option because of the availability of other medications with a better side effect profile.[22][23] Amongst the biologic agents, Rituximab, a monoclonal antibody against CD20 antigen, has been shown to provide sustained improvement in neutropenia without major side effects.[24][25] It can be considered in patients who fail to respond to an adequate trial of non-biologic DMARD therapy. Limited reports on anti-tumor necrosis factor agents like infliximab, adalimumab, and etanercept have not shown any benefit in neutrophil response.[25]
Initially, glucocorticoids can be used in patients with Felty syndrome to provide a rapid improvement in neutrophil count. Because of the immunosuppressive effect, however, long term use is generally not advised, and use should be avoided in patients with active infection.[26] Granulocyte colony-stimulating factor (G-CSF) is usually used in patients with absolute neutrophil count (ANC) of less than 1000/microliter with severe and recurrent infections who fail to respond to DMARDs and rituximab adequately. In a systemic review, all patients with FS receiving G-CSF had a significant increase in ANC within one week of treatment. In most of the patients, discontinuation of G-CSF resulted in the decline of ANC; however, it stabilized above a pre-treatment level over time. There was also improvement in infectious complications. During an active infection, short term treatment with goal ANC of over 1000/microliter can be beneficial. There will be an additional stimulatory effect on neutrophil function as well. Although long term G-CSF therapy has a risk of exacerbation of the underlying autoimmune condition, its use is a consideration in patients with severe recurrent infections with consistent ANC below 1000/microliter despite immunosuppressive therapy.[27]
Splenectomy in a patient with Felty syndrome was first tried by Hanrahan and Miller in a 50-year-old woman who had marked improvement in neutropenia and arthritis over five months follow up. After this, splenectomy was the main treatment option for Felty syndrome.[28][16] With the development of DMARDs and other biologic agents, the surgical approach has limited indications. It is reserved for patients who have significant recurrent infections with neutropenia and those who have failed to respond to all medical therapies, including DMARDs, biologic agents, and G-CSF. Other rare indications of splenectomy are severe anemia requiring multiple transfusions and severe hemorrhage due to thrombocytopenia which is not responsive to conventional treatment.[29]
Differential Diagnosis
The most important differential to consider in patients with RA and neutropenia is LGL leukemia. Also termed "pseudo-Felty syndrome," it can present as neutropenia with or without splenomegaly. Most patients with LGL leukemia have an associated autoimmune condition, particularly RA; therefore, it can be challenging to distinguish FS from LGL leukemia. Immunophenotyping showing cytotoxic T lymphocytes with CD 2, 3, 8, 16, and 57 surface marker positivity together with bone marrow biopsy and peripheral smear showing increased LGL cells can help in differentiating the two diseases. Many consider these two to be part of the same disease continuum rather than separate entities. The involvement of a hematologist to rule out hematological malignancy as the cause of neutropenia is important.
Other causes of neutropenia and splenomegaly should be evaluated and ruled out. Medications are an important cause to consider. Methotrexate can cause bone marrow suppression and neutropenia in patients with RA. Similarly, TNF inhibitors can cause neutropenia. Worsening of neutropenia after temporary cessation of these agents provides a clue to the diagnosis of Felty syndrome. Viral infections like EBV and HIV can present with neutropenia and splenomegaly. If suspected, serological tests can help rule out these conditions. Other autoimmune conditions such as lupus, which can have similar features as an extra-articular RA, can usually be distinguished through clinical features and serological tests.
Prognosis
The severity and extra-articular manifestations of RA has been decreasing gradually since the methotrexate, and biologic treatments became available for the treatment of RA.[5] The incorporation of G-CSF in the treatment of chronic neutropenia has resulted in decreasing need for splenectomy.[30] One study done before the advent of methotrexate reported 5-year mortality of 36% in patients with Felty syndrome, infections being the most common cause of death.[31] Recent data regarding the prognosis of FS is lacking. However, the availability of advanced treatment options has improved the prognosis for Felty syndrome.
Complications
The most important complication of Felty syndrome is severe or recurrent infections, particularly of respiratory tract and skin, because of neutropenia. Other complications like anemia due to splenic sequestration and hemorrhage due to severe thrombocytopenia can also occur. Variceal bleeding due to portal hypertension is possible. Treatment modalities like splenectomy for refractory neutropenia can increase the risk of infections post-surgery and have been fatal in a few cases. G-CSF carries a small risk of exacerbation of underlying autoimmune disorder.
Deterrence and Patient Education
Although it is a rare disease, Felty syndrome should be on the differential diagnosis of any patients who present with RA and neutropenia, because the consequence of any treatment delay is potentially fatal. The clinician should be mindful that neutropenia may become masked in patients with acute infection. No specific treatment exists for patients with Felty syndrome. Although many options are available for treatment, randomized trials are lacking because of the rarity of the disease. The basis for treatment recommendations is only a few observational studies. This diagnosis, therefore, poses a therapeutic challenge in an acute setting, especially in resource-limited situations and refractory neutropenia. In the non-acute settings, all patients with asymptomatic neutropenia should be advised about good oral and dental hygiene and should be closely monitored with adjustment in their anti-rheumatic medications to improve the neutrophil count, which can help prevent infections.
Enhancing Healthcare Team Outcomes
Felty syndrome is a rare disease, therefore a high degree of suspicion is required to make the diagnosis early and minimize its complications. The management of Felty syndrome should involve an interprofessional team. Apart from the involvement of a rheumatologist, a hematologist's input is valuable to rule out hematological malignancies as the cause of neutropenia. An infectious disease specialist should be involved earlier in the care to decrease the risk of infections.
The clinical pharmacist can assist the providers in monitoring hematologic parameters for the patient with RA, with or without therapy, to help in early detection of the disease and for the alteration of therapy when needed. The pharmacist should also assist the medical team by providing patient education on the different drugs used to treat Felty syndrome, their benefits, and adverse effects. Pharmacists need to verify dosing (particularly with MTX), check for drug interactions in the patient's medication regimen, and inform the clinician should they encounter any concerns.
The primary care nurse can help the providers make the diagnosis in patients with RA by obtaining a detailed interval history for possible recurrent infections, gastrointestinal bleeding, and splenic pain. Nurses can also assist the team in monitoring, verifying patient compliance, and helping assess treatment effectiveness.
Instituting a collaborative interprofessional team can help in the early detection and treatment of FS. Open communication between interprofessional team members across disciplines is vital to improving outcomes. [Level V]
(Click Image to Enlarge)
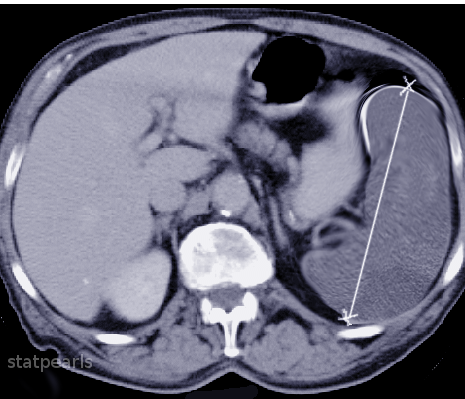
CT Splenomegaly
Image courtesy O.Chaigasame