Anatomy, Bony Pelvis and Lower Limb, Thigh Femoral Nerve
- Article Author:
- Nader Refai
- Article Editor:
- Prasanna Tadi
- Updated:
- 10/27/2020 8:45:02 AM
- For CME on this topic:
- Anatomy, Bony Pelvis and Lower Limb, Thigh Femoral Nerve CME
- PubMed Link:
- Anatomy, Bony Pelvis and Lower Limb, Thigh Femoral Nerve
Introduction
The femoral nerve is the largest nerve of the lumbar plexus. It forms from the dorsal divisions of the L2-L4 ventral rami.[1] It has a role in motor and sensory processing in the lower limbs. As a result, it controls the major hip flexor muscles, as well as knee extension muscles. It also controls sensation over the anterior and medial thigh, as well as medial leg down to the hallux. Therefore, it has several branches as it originates in the lumbar spine, down into the pelvis and further down into the lower limbs.
Structure and Function
In the Abdomen
The femoral nerve begins its course in the abdomen, by passing through the psoas major muscle. It then traverses laterally to the distal part of the psoas major muscle, and then finally, it runs “sandwiched” in between the iliacus muscle and the psoas major muscle.[2] The iliacus muscle is inferior to the femoral nerve, and the psoas major muscle is superior to the femoral nerve. It is at this point that two motor branches come off the femoral nerve, one to the psoas major and one to the iliacus muscle. These muscles will flex the hip.
In the Pelvis
The femoral nerve then enters the thigh. To do so, it must enter the femoral triangle by running inferior to the inguinal ligament. The femoral triangle is formed by three structures: sartorius (laterally), adductor longus (medially) and the inguinal ligament (superiorly).[3] Inside the femoral triangle exists the femoral nerve, femoral artery, femoral vein, femoral canal, and lymphatic vessels (in order from most lateral to medial).[4] About 4 cm below the inguinal ligament, the femoral nerve then divides into anterior and posterior divisions. The two divisions of the femoral nerve are distinguishable because the lateral femoral cutaneous artery splits them.[5]
Anterior Division
The anterior division of the femoral nerve has four terminal branches, two motor and two sensory. The motor branches are nerve to pectineus, nerve to sartorius. These muscles help to flex the hip as well.
The sensory branches of the anterior division are the medial cutaneous nerve of the thigh and the intermediate cutaneous nerve. These nerves are collectively responsible for the anteromedial sensory innervation of the thigh.
Posterior Division
The posterior division of the femoral nerve has a sensory nerve, four motor branches, and nerves to the hip and knee joints (articular branches). The sensory nerve is called the saphenous nerve and is the largest cutaneous branch of the femoral nerve. It is responsible for sensory innervation along the anteromedial and posteromedial aspect of the leg, into the medial foot.[6] The femoral nerve becomes the saphenous nerve when it passes through the adductor canal. It continues to travel along the medial aspect of the tibia until about halfway down the tibia, where it finally divides into two branches. One branch is more posterior and ends at the ankle. The other branch is more anterior and continues along the medial aspect of the foot and terminates at the hallux.
The four motor branches of the posterior division of the femoral nerve are nerves to the rectus femoris, vastus medialis, lateralis, and intermedius muscles. These muscles are the major knee extensors of the leg and are colloquially termed “quadriceps muscles.”
Lastly, branches from the posterior division of the femoral nerve also supply the knee, and hip joints termed articular joint nerves. The nerve to the rectus femoris supplies the hip, while all three nerves supply the knee joint to the vasti medialis, lateralis, and intermedius. The articular nerves innervate the fibrous capsule, ligaments, and synovial membranes of the joints, following Hilton’s law.[7]
Blood Supply and Lymphatics
The femoral nerve travels along with the femoral artery, vein, and lymphatics in the femoral triangle. The femoral artery and some of its branches supply the femoral nerve and its branches with oxygenated blood to maintain its function.
Nerves
Nerve to the psoas major
Nerve to Iliacus
Anterior Division:
- Motor:
- Nerve to sartorius
- Nerve to pectineus
- Sensory:
- The medial cutaneous nerve of the thigh
- The intermediate cutaneous nerve of the thigh
- Posterior Division:
- Motor:
- Nerve to rectus femoris
- Nerve to vastus medialis
- Nerve to vastus lateralis
- Nerve to vastus intermedius
- Articular:
- Hip - supplied by rectus femoris nerve
- Knee - supplied by all three vasti nerves
- Sensory:
- Saphenous nerve.
- Infrapatellar branches to the knee.
- Motor:
Muscles
Psoas major - major flexor of the hip
Iliacus - major flexor of the hip
Sartorius - flex, abduct, and laterally rotate the thigh at the hip. It can also flex and medially rotate the leg at the hip
Pectineus - flex and adduct the thigh at the hip
Physiologic Variants
In a case study in Karnataka, India, researchers observed that in a 65-year-old male cadaver, the left femoral nerve had split in the abdomen, when coming off of the L2-L4 nerve roots. It then rejoined to form the femoral nerve just proximal to the inguinal canal.[8]
Surgical Considerations
Surgeons use the femoral artery for arterial access in many procedures, including aortic aneurysm repairs.[9] It is essential to identify the femoral nerve before doing such a procedure, as damage to the nerve can result in loss of function of any of the muscles innervated by the femoral nerve.
Researchers have found the branches to the rectus femoris to range between 1 and 4 branches, with the most common innervation pattern being two branches. As a result, it is important to be aware and identify the possible variants and landmarks of the different possible branches.[10]
Clinical Significance
Radiculopathy and Loss of Reflexes
Radicular pain is irritation or inflammation of a nerve root. This is usually due to disc herniation. The symptoms include pain that travels in a dermatomal fashion. Motor deficits, as well as sensory deficits, can occur due to disc herniations.[11] If a disc herniation occurs on the L4 spinal nerve root, one can also lose their patellar reflex because reflexes include an afferent and efferent limb, which are affected in radicular pain.
Femoral Hernia
Femoral hernias are less likely to occur than inguinal hernias, however, they are more likely to occur in elderly females. They are protrusions of abdominal contents through a weakening in the femoral canal. They create a bulge in the groin area and can lead to strangulation and necrosis of abdominal contents if not treated. Due to being located in the femoral canal, laterally will be the femoral vein.[12]
Psoas Abscess/Hematoma
Any kind of infection or hematoma can cause a mass effect injury near the psoas muscle or iliacus muscle. Due to the relative location of these muscles to the femoral nerve, the growing abscess or hematoma can begin to compress the femoral nerve. This can lead to nerve injury, which can affect motor or sensory innervation from the femoral nerve.[13]
Femoral and Saphenous Nerve Blocks
Femoral nerve blocks are common in the management of hip pain in hip fracture patients; this is because it avoids opioid side effects and addictive properties. Pericapsular nerve group (PENG) blocks target articular branches of the femoral nerve to alleviate pain in the hip.[14]
Femoral Nerve Damage
- The most common etiology is direct sharp trauma.
- A compressive etiology can damage the nerve due to ischemia such as hematoma or tumor.
- Iatrogenic injuries have been reported following intraabdominal operations and hip surgeries due to prolonged compression, retraction, or stretching of the nerve.[15]
- Proximal interlocking screw placement through femoral IM nailing can be a risk factor for iatrogenic injury of the femoral nerve.
- Although uncommon, femoral nerve neuropathy has been reported in complex anterior and posterior spinal surgery [16].
Clinically, patients will have quadriceps wasting, loss of knee extension, and to a lesser extent hip flexion due to the involvement of iliacus and pectinues muscles. On the sensory side, there will be loss of sensation over the front and medial side of the thigh due to the involvement of the anterior and medial cutaneous nerves of the thigh. Also, loss of sensation over the medial aspect of the lower leg and foot due to the involvement of the saphenous nerve. Although the prognosis in most cases is satisfactory, some cases will necessitate nerve repair or grafting and some cases will end up with permanent residual neurologic deficits.
(Click Image to Enlarge)
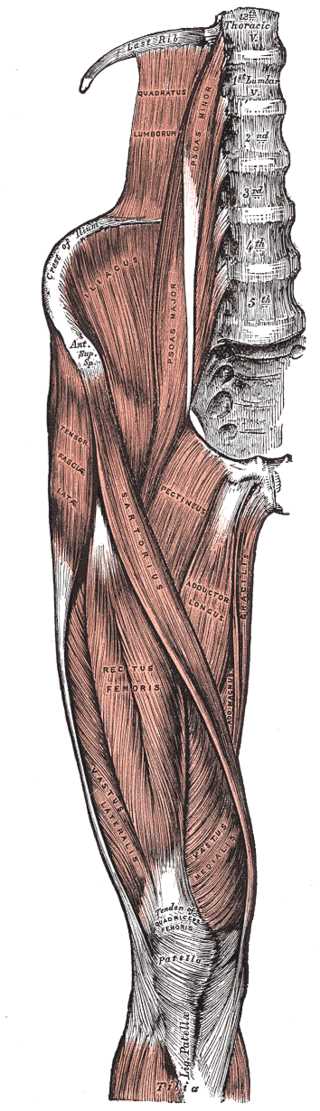
Tensor Fasciae Latae Muscles, Abductor of the Thigh, Thoracic Vertebrae, Quadratus Lumborum, Psoas Minor and Major, Crest of Ilium, Anterior Superior Spine, Iliacus, Tensor Fascia Latae, Sartorius, Pectineus, Adductor Longus, Gracilis, Adductor Magnus, Rectus Femoris, Vastus Lateralis and Medialis, Tibia, Patella, Tendon of Quadriceps
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)

Femoral Canal Arteries and Veins, Great saphenous veins, Femoral Nerve
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)
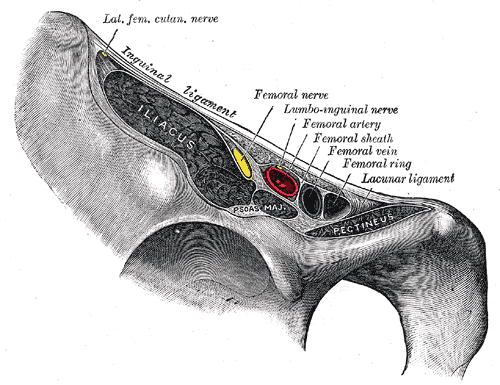
Vascular Lacuna, Femoral Nerve, Ilioinguinal nerve, Femoral sheath, Femoral artery, Femoral vein and ring
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)

Nerve Roots L2-L4 joining to form Femoral Nerve
Contributed by Grays Anatomy Plates (Public Domain
(Click Image to Enlarge)
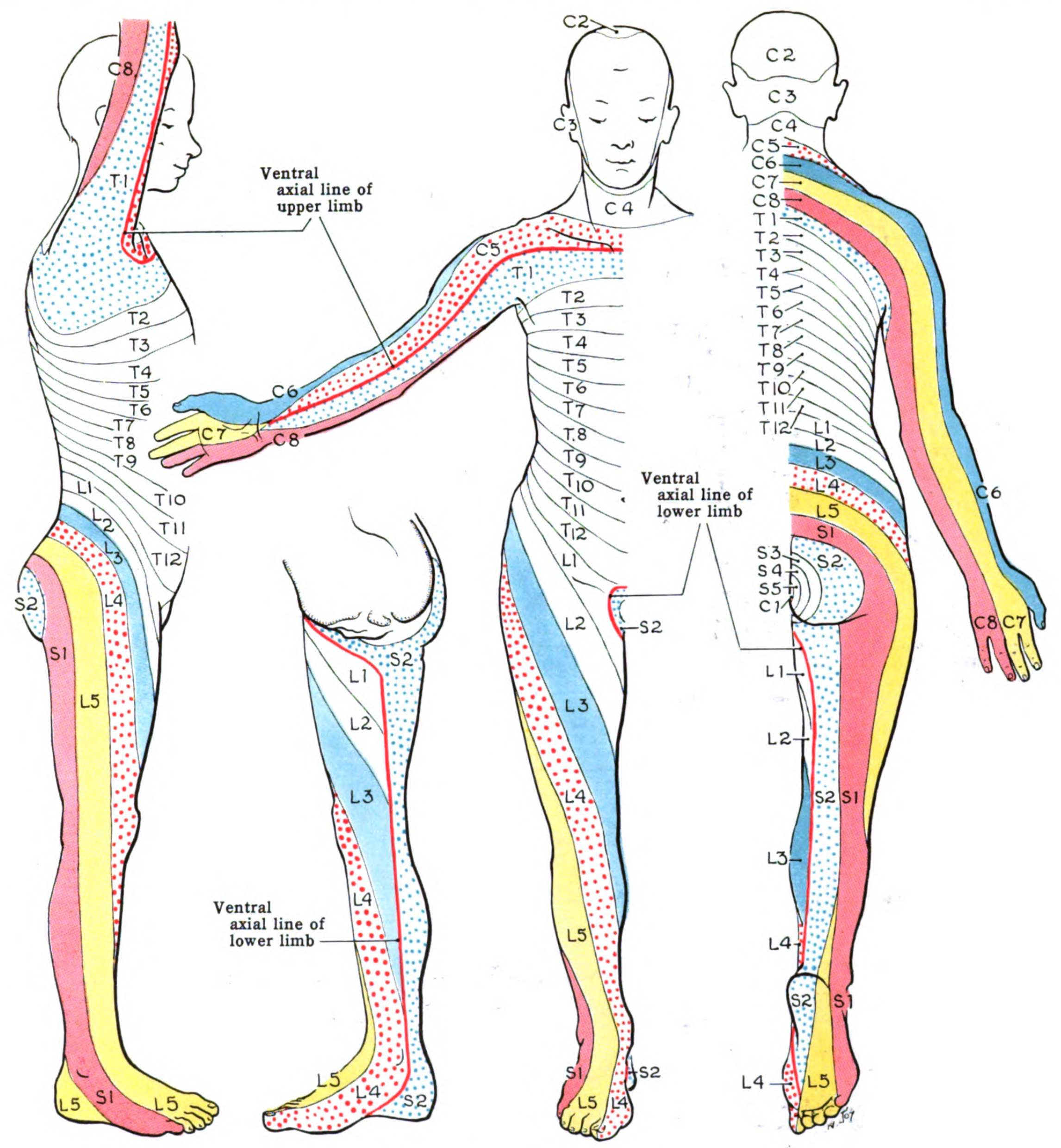
Dermatome Map distribution of L2-L4
Contributed from Wikimedia. Grant, John Charles Boileau (Public Domain) An atlas of anatomy, by regions 1962