Anatomy, Shoulder and Upper Limb, Hand Flexor Digitorum Profundus Muscle
- Article Author:
- Brandon Lung
- Article Editor:
- Bracken Burns
- Updated:
- 11/2/2020 7:01:32 AM
- For CME on this topic:
- Anatomy, Shoulder and Upper Limb, Hand Flexor Digitorum Profundus Muscle CME
- PubMed Link:
- Anatomy, Shoulder and Upper Limb, Hand Flexor Digitorum Profundus Muscle
Introduction
The flexor digitorum profundus (FDP) is an extrinsic hand muscle that flexes the metacarpophalangeal and distal interphalangeal joints of the index, middle, ring, and little fingers. The flexor digitorum profundus lies in the deep volar compartment of the forearm and originates from the upper three-fourths of the volar and medial surfaces of the ulna, interosseous membrane, and deep fascia of the forearm. The tendons of the flexor digitorum profundus insert into the base of the distal phalanges of the index, middle, ring, and little fingers. The tendons of the flexor digitorum profundus lie deep to the tendons of the flexor digitorum superficialis, and the tendon to the index finger is usually separate from the other three partially attached flexor digitorum profundus tendons as they pass through the carpal tunnel.[1] Since the tendons of the flexor digitorum profundus arise at or below the wrist joint, contraction of the muscle produces mass action movement in all four tendons and allows for a power grip.
Structure and Function
The flexor digitorum profundus is a flexor of the midcarpal (wrist), metacarpophalangeal, and interphalangeal joints of the index, middle, ring, and little fingers. Since the lumbricals arise from the flexor digitorum profundus tendons and insert into the dorsal extensor expansions of the proximal phalanges, the flexor digitorum profundus muscle aids the lumbricals in fully extending the fingers at the interphalangeal joints and flexing the fingers at the metacarpophalangeal joints. Flexion at the distal interphalangeal joints depends on wrist positioning and the tension generated at the distal joints is reduced when the wrist is fully flexed.
Embryology
The upper limb musculature is derived from the dorsolateral cells of somites that migrate into the limb around the fourth week to form muscles. With elongation of the limb buds, the muscle tissue splits into flexor and extensor components determined by connective tissue derived from the lateral plate mesoderm. The zone of polarizing activity at the posterior border of the upper limb secretes sonic hedgehog to control anterior-posterior patterning.[2] Once the limb bud forms, the ventral primary rami penetrate into the mesenchyme, and the median and ulnar nerves are formed by the ventral branch to eventually supply the flexor digitorum profundus.
Blood Supply and Lymphatics
The flexor digitorum profundus is supplied by the anterior interosseous artery, which is a branch of the common interosseous artery. The anterior interosseous artery is accompanied by the palmar interosseous branch of the median nerve and gives off muscular branches to the flexor digitorum profundus and flexor pollicis longus muscles. The flexor digitorum profundus lymphatic drainage is part of the upper limb lymph system, consisting of superficial and deep lymphatic vessels. The superficial vessels around the basilic vein go to the cubital lymph nodes, which are proximal to the medial epicondyle of the humerus. Vessels around the cephalic vein go to the axillary lymph nodes. The deep lymphatic vessels also drain lymph from the flexor digitorum profundus and follow the major deep veins, eventually terminating in the humeral axillary lymph nodes.
Nerves
The lateral part of the flexor digitorum profundus muscle (associated with the index and middle fingers) is innervated by the anterior interosseous branch of the median nerve, and the medial part of the muscle (associated with the ring and little fingers) is innervated by the ulnar nerve (C8, T1). Besides the flexor carpi ulnaris, the flexor digitorum profundus is the only flexor muscle that is not exclusively innervated by the median nerve.
The median nerve descends between the flexor digitorum superficialis and the flexor digitorum profundus proximally. The anterior interosseous nerve branches from the median nerve halfway down the forearm and from the dorsal lateral aspect of the median nerve. The anterior interosseous nerve has only motor functioning.
Muscles
Along with the flexor pollicis longus and pronator quadratus, the flexor digitorum profundus muscle forms the deep layer of the ventral forearm muscles. The decussation of the flexor digitorum profundus tendons and the flexor digitorum superficialis (FDS) tendons occurs at the Camper chiasm.[3]
Physiologic Variants
The flexor digitorum profundus physiologic variants are causes of spontaneous flexor tendon ruptures as described in the literature. The two ulnar flexor digitorum profundus tendons usually originate from the same muscle belly and separate in the forearm or carpal tunnel. However, several case reports have described a variant of the flexor digitorum profundus little finger tendon in which the tendons of the little and ring finger are fused together at the midpalmar level.[4] This anatomic anomaly predisposes to flexor digitorum profundus tendon rupture as the little finger tendon is at the weakest point against shearing forces from the pulling stress.
Surgical Considerations
The volar approach to the flexor tendons is important for the best possible exposure of the flexor tendons within their fibrous sheaths. This approach is used for exploration and repair of the flexor digitorum profundus tendons, repair of digital nerves and vessels, and exposure of the fibrous flexor sheaths for drainage of pus.
Operative treatment for avulsion injury of the flexor digitorum profundus (jersey finger) includes direct tendon repair, tendon reinsertion with a dorsal button, open reduction internal fixation of the fracture fragment, two-stage flexor tendon grafting, and distal interphalangeal arthrodesis.[5] Direct tendon repair and tendon reinsertion with a dorsal button is done in an acute injury setting (greater than 3 weeks) and prevents the risk of distal interphalangeal (DIP) flexion contracture or quadrigia if greater than 1 cm advancement of the flexor digitorum profundus tendon is not corrected. Open reduction internal fixation of the fracture fragment is done for large avulsion fractures with associated retraction of the tendon either to the DIP joint or into the palm. Two-stage flexor tendon grafting of the flexor digitorum profundus is indicated for chronic injury (greater than 3 months) with a full passive range of motion of the DIP joint. DIP arthrodesis is a salvage procedure in chronic injury with chronic stiffness.
Clinical Significance
Injury to the flexor digitorum profundus tendon distal to the lumbrical origin by rupture or amputation can cause lumbrical plus finger, which manifests as a paradoxical extension of the interphalangeal joints when attempting to flex the finger.
Since the flexor digitorum profundus tendons to the small, ring, and long fingers have a common muscle belly, the tendons may not be able to move independently if they are interconnected with the separate tendon that runs to the index finger. This condition is known as quadrigia, in which one set of tendons will not have full excursion if the other set of tendons becomes shorter. Quadrigia results in the patient not being able to make a full fist and an associated weak grasp.[6]. Loss of flexion in the other digits occurs when the tendon is not shortened to the same length as the other set of tendons. Quadrigia due to tendon shortening has many etiologies, including adhesion or scarring of the flexor digitorum profundus tendons. Overtightening and distal advancement of the flexor digitorum profundus tendons after rupture and repair may also lead to quadrigia. Flexor digitorum profundus tendon amputation and suturing to the extensor tendons may also lead to quadrigia and loss of digit flexion.
Rupture of the flexor digitorum profundus tendon from the distal attachment insertion at the base of the distal phalanx is known as jersey finger. Jersey finger is a zone 1 flexor tendon injury that involves the ring finger in 75% of cases. The flexor digitorum profundus muscle belly is in maximal contraction during forceful distal interphalangeal joint extension. Classification of a flexor digitorum profundus tendon avulsion injury is based on the Leddy and Packer classification, which stratifies the injuries based on the level of tendon retraction and presence of a fracture. Patients presenting with jersey finger may complain of pain and tenderness over the volar distal finger with no active flexion of the distal interphalangeal joint. At rest, the affected finger lies in slight extension relative to the other fingers, and the proximally retracted flexor tendon may be palpated along the flexor sheath. Jersey finger is a common cause of quadrigia, in which a greater than 1 cm advancement of the flexor digitorum profundus tendon increases the risk of distal interphalangeal joint flexion contracture.
In anterior interosseous nerve injury, the patient will be unable to perform an “OK” sign with the thumb due to paralysis of the flexor pollicis longus and the flexor digitorum profundus muscles to flex the DIP joint.
Other Issues
In cases of compartment syndrome seen in supracondylar, ulnar, or radius fractures, the volar compartment of the forearm is released. Volar compartment syndrome presents as pain with passive extension of the fingers and wrist, tenderness over the volar aspect of the forearm, flexion posture of the fingers, and weakness of finger and wrist flexion. Fasciotomy of the forearm is performed, and both the superficial and deep volar compartments must be released.
(Click Image to Enlarge)
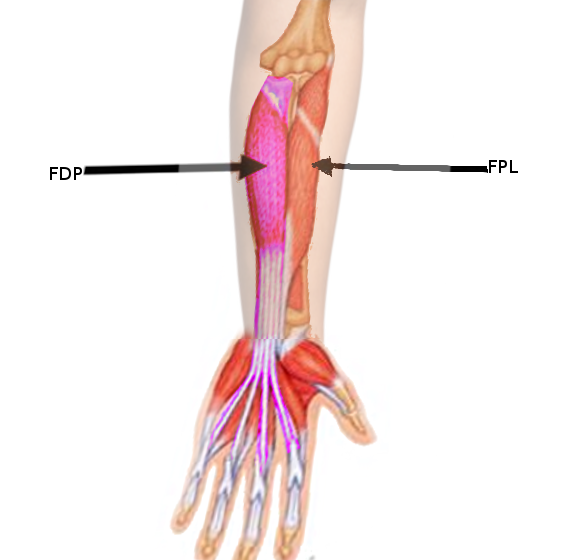
Flexor digitorum profundus
Image courtesy S Bhimji MD
(Click Image to Enlarge)

Flexor digitorum superficialis
StatPearls Publishing Illustration