Hypothyroid Myopathy
- Article Author:
- Maria Fariduddin
- Article Editor:
- Nidhi Bansal
- Updated:
- 8/12/2020 3:13:29 PM
- For CME on this topic:
- Hypothyroid Myopathy CME
- PubMed Link:
- Hypothyroid Myopathy
Introduction
Hypothyroid myopathy is a common clinical feature in patients with hypothyroidism affecting about 79% of patients. It is seen in both congenital and acquired hypothyroidism, and generalized myalgias and muscle weakness characterize it. Patients with severe or untreated hypothyroidism can develop significant muscle disease leading to severe functional limitations. [1]
Etiology
Hypothyroid myopathy is a complication of uncontrolled on untreated hypothyroidism. It is seen in both congenital and adult forms of hypothyroidism and sometimes is the presenting feature of subclinical hypothyroidism.
Epidemiology
Women are affected by this disease more frequently than men, and it can be seen at any age. Studies report a range of 40 to 70 years. No predilection for any particular race has been noted.
Pathophysiology
The pathogenesis of myopathy in hypothyroidism is not well understood. Thyroid hormones have a significant influence on cellular metabolism, and their deficiency causes impairment of the normal functioning of the cell. Thyroxine (T4) deficiency leads to a reduced mitochondrial oxidative capacity, abnormal glycogenolysis and an insulin resistant state of the cell. This leads to selective atrophy of type 2 muscle fibers (fast-twitching type) as they are dependent on glycolysis for energy causing the slowing of muscle contraction seen clinically in patients with hypothyroidism. Muscle hypertrophy ensues as a result of this, which is believed to be a compensatory response that happens from the accumulation of glycosaminoglycans in the muscle. Increase in connective tissue and muscle fibers also contributed to this hypertrophy. There is also a decrease in muscle carnitine in patients with thyroid dysfunction causing myopathic symptoms. The muscle involvement in hypothyroidism is caused by alterations in muscle fibers from fast-twitching type 2 to slow-twitching type 1 fibers, deposition of glycosaminoglycans, poor contractility of actin-myosin units, low myosin ATPase activity and low ATP turnover in skeletal muscle.
It has been noted that the degree of muscle weakness does not always correlate with the severity of thyroid hormone deficiency and this suggests that besides impaired muscle function, structural muscle injury might have a role in the pathogenesis of the myopathy in some cases. Muscle cell membrane permeability changes can lead to serum muscle enzyme elevations in the absence of symptoms or structural abnormalities, and reduced clearance of these enzymes can contribute to the muscle injury as well. Animal studies have shown the involvement of thyroid hormone in regulating gene expression of skeletal muscle proteins like myosin ATPase strengthening the role of thyroid hormone deficiency in the pathogenesis of hypothyroid myopathy. [1],[2],[3]
History and Physical
Hypothyroid myopathy presents with nonspecific symptoms of myalgias, muscle cramps, fatigue, and muscle weakness, particularly exacerbated with exertion and exercise. Proximal weakness especially in the shoulder and pelvic girdle is commonly seen, causing difficulty in climbing stairs, getting up from squatting position, and combing hair. The severity of myopathy correlates with the duration and degree of thyroid hormone deficiency. Diffuse muscle hypertrophy is a relatively rare phenomenon. [4]
There are 4 subtypes of myopathy associated with hypothyroidism: myasthenic syndrome, atrophic form, Kocher-Debre-Semelaigne syndrome, Hoffman syndrome.
- Myasthenic syndrome is associated with ptosis and severe weakness beginning in childhood that can progress to loss of mobility in later life.
- Severe muscle atrophy is seen in the atrophic form of hypothyroid myopathy.
- Kocher-Debre-Semelaigne syndrome is seen in childhood and is associated with generalized muscular hypertrophy, myxoedema, short stature, and cretinism.
- Hoffmann syndrome is usually seen in adults and characterized by pseudohypertrophy, painful spasms, proximal muscle weakness, and stiffness. This is generally seen in primary hypothyroidism and very rarely with secondary hypothyroidism. The cause of muscle pseudohypertrophy in Hoffmann’s syndrome is complex and largely unclear. It is postulated to be due to deposition of glycosaminoglycans and increased muscle fiber size. The muscles commonly involved are the tongue, arm and leg muscles. [5]
Rhabdomyolysis is, fortunately, a rare complication of severe and untreated hypothyroid myopathy, but can be life-threatening. Common precipitating factors are vigorous exercise, trauma, electrolyte abnormalities, and alcohol consumption.
Acute compartment syndrome may also be seen with delayed tendon reflexes and muscle hypertrophy, especially when precipitated by trauma, thrombosis, animal bites, intravenous (IV) drug abuse or surgery.
Myoedema is an interesting clinical sign, characteristic of hypothyroid myopathy. It is demonstrated by percussion or a pressure stimulus on the muscles of the arm. This causes the muscle to form a palpable, painless ridge around the site of the stimulus. The swelling subsides gradually returning the muscle contour to normal in a few seconds. This is believed to be caused by prolonged muscle contraction due to delay in calcium reuptake by the sarcoplasmic reticulum after the stimulus causes local calcium release. This sign if elicited can help differentiate hypothyroid myopathy from other types of myopathies.
Evaluation
Hypothyroidism is a prerequisite for the diagnosis of hypothyroid myopathy and is diagnosed by measurement of thyroid-stimulating hormone (TSH) and T4 levels in the blood. Most common laboratory finding in the patients' hypothyroid myopathy is the elevation of creatine kinase (CK) in the serum. This is not specific for myopathy and patients may have an elevation of CK for many years prior to developing the myopathy.
Electromyography (EMG) can demonstrate low/small amplitude potentials which could help with diagnosis. However, it is normal in half of the patients and does not preclude the diagnosis. Myoedema is electrically silent as well and helps distinguish myotonia on an EMG. When compared with myositis, there is a lack of fibrillation potentials on EMG with relatively normal motor units. [2]
Muscle biopsy is not necessary for diagnosis but if done, will show swollen and pale muscle tissue with loss of striations and increased separation between the muscle fibers due to mucinous depositions. Type I muscle fiber hypertrophy, type 2 muscle fiber atrophy or focal necrosis and degeneration of muscle fibers may also be noted. Increased numbers of internal nuclei, mitochondrial inclusions, glycogen accumulation, autophagic vacuoles and myofibrillar disorganization are some other non-specific histopathological features that could be seen on the muscle biopsy. [4]
Treatment / Management
Management of hypothyroidism is the mainstay of treating hypothyroid myopathy. It is reversible with timely diagnosis and prompt treatment. [6][7]
With adequate thyroid hormone replacement and restoration of normal thyroid function, gradual resolution of most neuromuscular symptoms is noted in most of the patients. CK levels fall quickly with thyroxine replacement with a few weeks and could resolve even before TSH comes to a normal range. Hence, this can be used as a surrogate to monitor response to treatment in the initial stages, as the myopathic symptoms can take up to 6 months to resolve. Most of the symptoms resolve within a year of adequate hormone replacement. [4],[8][9][10]
Differential Diagnosis
- Acid maltase deficiency
- Acute poliomyelitis
- Amyotrophic lateral sclerosis
- Becker muscular dystrophy
Enhancing Healthcare Team Outcomes
Hypothyroid myopathy is fairly common but often missed because clinicians fail to ask patients about muscle-related symptoms. It is often mistaken for fatigue. The condition is best managed by an interprofessional team that includes a pharmacist, orthopedic nurse, therapists, and physicians. The key it to replace the thyroid hormone, encourage physical activity, and enroll in a physical therapy program.
The recovery is not immediate and may take months or even several years. The patient should be monitored by serial CK levels. Even after treatment, residual muscle pain and fatigue may persist in some patients. Nursing staff should assist with monitoring, followup, and education of the patient and family. [Level 5]
(Click Image to Enlarge)
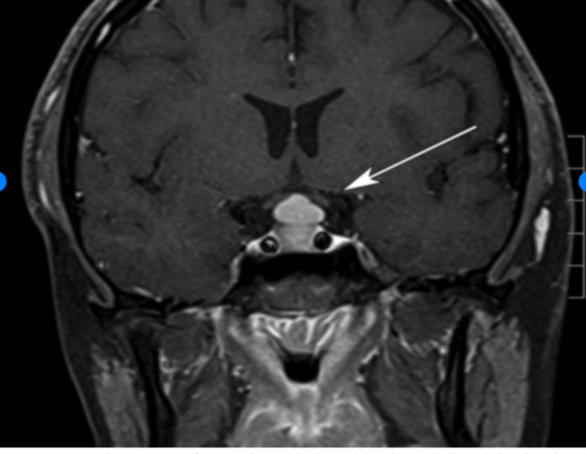
Tablets or scalpel: Pituitary hyperplasia due to primary hypothyroidism
Contributed from Ahmed Imran Siddiqi MBBS, MRCP Stephanie E. Baldeweg MD, FRCP, FRCP Et al Radiology Case Reports ,Volume 10, Issue 2, 2015, 1099