Keratosis Pilaris
- Article Author:
- Keith Pennycook
- Article Editor:
- Tess McCready
- Updated:
- 6/29/2020 1:26:46 AM
- For CME on this topic:
- Keratosis Pilaris CME
- PubMed Link:
- Keratosis Pilaris
Introduction
Keratosis pilaris is among the most common dermatologic conditions and can be considered a normal variant. It is the most common follicular keratosis. The condition is multifactorial and innocuous, affecting the extensor surfaces of the proximal extremities. Keratosis pilaris first appears in early childhood and progresses, becoming most extensive during the second decade of life. Keratosis pilaris is associated with many other conditions, including atopic dermatitis, ichthyosis vulgaris, obesity, diabetes mellitus, and malnutrition. It can also present in conjunction with syndromes such as Down syndrome and Noonan syndrome.[1] The condition often improves over time, but several treatment options are available. Emollients, exfoliants, antiinflammatory medications, phototherapy, and various laser therapies can be used to treat keratosis pilaris.[2]
Etiology
Although keratosis pilaris is a common condition, the exact etiology remains unknown.[3] The condition has an autosomal dominant mode of inheritance.[4] Mutations in filaggrin have correlations with keratosis pilaris as well as abnormalities of the Ras signaling cascade.[5][6] The follicular abnormalities seen in keratosis pilaris may result from mutations in the filaggrin gene.[4] Keratosis pilaris is most commonly associated with atopic dermatitis. This association, as well as mutations in the filaggrin gene, suggests keratosis pilaris is the result of a loss of normal epithelial barrier function.[7]
Epidemiology
Keratosis pilaris is a common dermatologic condition. The most common patient population is adolescents, with 50 to 80 percent affected. The disorder is also frequently seen in adults, with 40 percent of the adult population affected.[4] However, because keratosis pilaris is an underreported condition, the prevalence of the condition may be higher.[3] Race and sex do not predispose patients to develop keratosis pilaris.[8]
Pathophysiology
Similarly to the etiology, there is no well-established pathophysiology of keratosis pilaris. The most widely accepted theory proposes abnormal follicular epithelial keratinization causing an infundibular plug to form.[7] These keratotic plugs lead to erythema and scaling around the follicle opening.[6][4] The keratin plugs also result in the formation of inflammatory papules which are a hallmark characteristic of keratosis pilaris.[5] Furthermore, coiled hairs are present within the lesions and may play a role in the inflammation and keratinization of keratosis pilaris.[7]
Histopathology
A punch biopsy is usually not indicated or necessary to make a diagnosis of keratosis pilaris. However, if a pathologist chose to perform a punch biopsy of a lesion, histology would display the following features: marked follicular plugging of the hair follicle orifice, with hyperkeratosis and acanthosis of the epidermis. Lymphocytic infiltrate of the dermis will also be present, and hypergranulosis may also present in this skin condition.[5]
History and Physical
A thorough history and physical exam are integral to making a diagnosis of keratosis pilaris. The physician should investigate the onset, appearance, location, and symptoms of the epidermal lesions. Inquiring about home treatments and how the condition is affecting the patient are also important steps in the management of keratosis pilaris. This skin condition most commonly presents in teenagers and correlates with atopic dermatitis.[7] Those affected by keratosis pilaris will present to the office complaining of red bumpy skin without pain or pruritus. This asymptomatic eruption generally occurs on the extensor surfaces of the proximal upper and lower extremities as well as the buttocks. However, the face, trunk, and distal extremities may also be involved.[6][7][9] The physician should look for numerous small inflammatory papules with follicular involvement in the typical locations.[3] Erythema and edema may accompany some lesions if the patient has been manipulating the papules to express the keratotic material. Psychological distress from the appearance of the lesions may prompt patients to seek care rather than symptoms from the lesions themselves.[4]
Evaluation
Keratosis pilaris is a clinical diagnosis based on history and physical exam findings. However, evaluation of the skin lesions with a dermatoscope can aid in the diagnosis. Abnormalities of the hair follicle will be displayed when visualizing the papules with a dermatoscope. Hair shafts can be thin and short, coiled, or embedded within the stratum corneum. Scaling and erythema will also be present on dermoscopy.[5] As stated above, a biopsy is generally not necessary for diagnosis.
Treatment / Management
Keratosis pilaris is an asymptomatic condition that generally improves over time. As a result, the treatment of the disease is unnecessary. However, patients can aid in the resolution of skin lesions by maintaining adequate hygiene, using hypoallergenic soaps, and abstaining from manipulating the papules. For patients interested in treatment, topical medications can be used to treat keratosis pilaris. The topical treatments include emollients and topical keratolytics. Skin texture improves with the use of either salicylic acid lotion 6% or urea cream 20%.[6] Other less common treatment options include laser treatments, retinoids, and vitamin D3 derivatives.[7] Although these treatments may provide a cosmetic benefit, there are no controlled clinical trials or a cure for keratosis pilaris.[4]
Some case reports have found success with the use of the topical retinoid, 0.01% tazarotene. When applied nightly, keratosis pilaris faded in two weeks and resolved after four to eight weeks.[10] Moreover, chemical peels utilizing 70% glycolic acid for 5 to 7 minutes have also been found to be useful in improving the appearance of keratosis pilaris.[11] Finally, multiple case reports have been published describing the use of lasers in the treatment plan of keratosis pilaris. Some clinicians have found success with pulsed dye laser, alexandrite laser, Nd:YAG laser, and fractional CO2 laser treatments.[12][13][14]
Differential Diagnosis
- Folliculitis
- Atopic dermatitis
- Milia
- Acne vulgaris
- Scurvy
Prognosis
Generally, keratosis pilaris develops during childhood and improves over time.[3] A study examining the course of keratosis pilaris determined 35 percent of patients improved over time, while 43 percent of patients had persistence of their condition. Keratosis pilaris worsened over time in twenty-two percent of patients. The severity of the condition can also vary with the changing of seasons. Forty-nine percent of patients saw improvement during the summer, and 47 percent saw a worsening of their presentation during the winter months.[15] These changes are most likely attributable to the reduced moisture content of the air during the winter months.
Complications
Complications of keratosis pilaris are limited and not well documented in the literature. Patients are often distressed about the cosmetic appearance of the condition.[4] Another complication that can occur is scarring secondary to the patient traumatically rupturing the lesions. Physicians must educate patients on the necessity to use the prescribed topical medications and refrain from manipulating the lesions.
Deterrence and Patient Education
Patient education is crucial for the proper management of keratosis pilaris. Patients need to understand the condition is chronic, and there is no cure for keratosis pilaris. The physician should also explain to the patient that the condition often improves over time without treatment, and treatments are for cosmetic purposes. Patients need to grasp that keratosis pilaris is often refractory to the available treatment options.[3] Due to the lack of evidence supporting treatments and often the lack of response to treatment, physicians should counsel patients on the risks and benefits of treating the condition.[8]
Enhancing Healthcare Team Outcomes
It is crucial for clinicians to provide patients with expectations for treatment success. Patients need to understand that treatment is difficult, but should receive reassurance that keratosis pilaris usually improves gradually as the patient ages. Clinicians should use a stepwise approach when treating this condition. Initial treatment options consist of emollients and topical keratolytics. If the patient shows no response to a trial of treatment, physicians should inform patients of other treatment options. Therapy can escalate to retinoids, topical anti-inflammatories, and Vitamin D3 derivatives. Phototherapy and multiple laser treatment modalities are also possible therapeutic options. Consider a dermatology referral for patients with keratosis pilaris that does not respond to treatment. Nursing can assist the clinicians by providing a significant role in patient counseling and monitoring treatment progression, informing the physician of any possible issues. As treatment ramps up to higher levels, the pharmacist becomes more involved, both in verifying the agents and administration instructions, but also assuming a counseling role for administration, and ensuring that there are no interactions in the patient's regimen, particularly with retinoid therapy. Even though the disease is relatively benign and self-limiting, it does not obviate the need for an interprofessional team approach, which will direct management for optimal patient results. [Level 5]
Finally, thorough education of the patient is vital; even though many treatments are available none works well or is consistently effective; since the condition is not life-threatening, patients need to understand that some treatments are more likely to cause harm than good. [Level 5]
(Click Image to Enlarge)
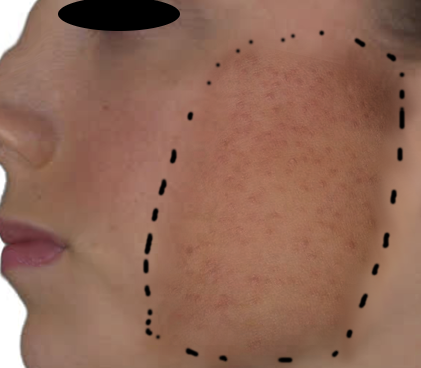
Keratosis pilaris
Image courtesy O.Chaigasame