Lumbosacral Discogenic Syndrome
- Article Author:
- Sanket Pathak
- Article Editor:
- Till Conermann
- Updated:
- 7/10/2020 4:09:19 PM
- For CME on this topic:
- Lumbosacral Discogenic Syndrome CME
- PubMed Link:
- Lumbosacral Discogenic Syndrome
Introduction
Low back pain is a common cause of disability among the general population with a well-documented cost burden placed on the U.S. healthcare system. There are multiple sources of chronic low back pain, often divided into whether the pain is facet-mediated, secondary to fracture, or discogenic in nature. This article will focus on the pathophysiology, evaluation, and treatment of lumbosacral discogenic syndrome and pain arising from pathology involving the intervertebral disc.
Intervertebral discs are pads of fibrocartilage that sit between the spinal vertebrae, occupying roughly one-third of the height of the spinal column.[1] Their major role lies in the transmission of mechanical loading from body weight and muscle activity, allowing bending, flexion, and torsion of the bony spine.
Each disc consists of two main components: a central, gel-like substance called the nucleus pulposus, and an outer, firmer annulus fibrosis. The consistency of the nucleus is a result of its water and proteoglycan content and is held together by a network of type II collagen and elastin fibers. The high anionic glycosaminoglycan content of this network gives the nucleus pulposus its osmotic properties, which allow it to resist compression. The annulus fibrosis is composed of bundles of type I collagen arranged in multiple oblique layers called lamellae. Characteristics of a normal, healthy disc demonstrate high water content in the nucleus and inner annulus. The most outer annulus provides tensile strength. Specifically, in the lumbar region, a healthy disc is typically 7-10 mm thick and 4 cm in AP diameter with approximately 20 layers of lamellae.[1]
The interverbal discs are supplied by the sinuvertebral nerve (SVN), which innervates the posterior annulus and posterior longitudinal ligament. In healthy subjects, the neural penetration of the annulus is about 3 mm, which corresponds to the outer three lamellae. It is a mixed nerve, containing a somatic root from the ventral ramus, as well as an autonomic root from the grey ramus. Once the nerve takes a recurrent course through the intervertebral foramen and enters the spinal canal, it divides into superficial and deep networks. The superficial network branches to multiple vertebral levels and contains mostly sympathetic fibers, while the deep network contains primarily somatic fibers and innervates the corresponding segment.[2]
The intervertebral discs are relatively avascular with the nucleus and inner annulus being supplied by capillaries that arise in the vertebral bodies and terminate at the bone-disc junction. Nutrients and small molecules such as glucose and oxygen reach the disc cells by diffusion.[3] Additionally, only the outermost portion of the annulus is vascularized. As a result, intervertebral discs are very limited in their ability to heal from injury, and, as a result, the healing process is overtaken by degenerative changes. This is not just due to avascularity, however, but also due to decreased cell population, which diminishes the structure’s ability to break down and turn over large collagen bundles.
Axial back pain may be of discogenic origin; however, not all damaged or degenerated discs cause pain. Disc abnormalities are commonly seen on MRI in asymptomatic individuals. Considered in the setting of other possible etiologies of axial low back pain with similar clinical presentation, this presents a challenge to the treatment provider.
Etiology
It is important to distinguish the difference between age-related changes and disc degeneration. After young adulthood, as nucleus cell density decreases, and the proportion of senescent cells increases, there is an accompanying decrease in proteoglycan content, disc water content, and extracellular matrix turnover.[4] As a result, the annulus becomes stiffer and must resist compression directly.
An additional finding can be the detachment of the hyaline cartilage endplates due to this loss of internal pressure. The nucleus also tends to bulge into the vertebral body leading to radial bulging of the annulus with subsequent loss of disc height. As a result, compressive stress is placed on the neural arches, leading to facet osteoarthritis and osteophyte formation. This can lead to another source of axial back pain. Other features of aging are a decrease in vertebral endplate permeability and metabolite transport. This is a noteworthy difference from disc degeneration where damage leads to an increase in these features.
Adams et al. define disc degeneration is an aberrant, cell-mediated response to progressive structural failure. Along with structural failure are signs of accelerated or advanced aging. Causes of disc degeneration include genetic inheritance, advanced age, inadequate metabolite transport, and loading history. These elements provide the setting for structural failure to occur with normal activities of daily living.[4]
Characteristics of structural damage include endplate fracture, radial fissure, and herniation. Due to the lumbar spine’s function as a major motion segment, annular disc tearing is more commonly seen in this region. There are three types of annular tearing. Circumferential tearing results from shear stress. Peripheral tearing usually is located in the anterior annulus and likely related to trauma. Radial tearing is associated with nucleus degeneration and posterior projection. If the nucleus migrates enough to affect the periphery, the disc is herniated or prolapsed. The extent of migration can result in protrusion, extrusion, or sequestration of the disc material. Additionally, damage or fracture to the vertebral endplate induces the increased activity of degradative enzymes and proapoptotic factors.[5]
Epidemiology
Lumbar intervertebral discs are shown to be a source of chronic back pain in 26% to 42% of patients with disc herniation [6]. Disc tearing is more common in the lumbar spine, peaking at middle age. Determining the prevalence of intervertebral disc degeneration is difficult, as most cases are asymptomatic. A systematic review performed by Brinjikji et al. looked at asymptomatic patients who underwent lumbar MRI and found that the prevalence of disc degeneration ranged from 37% of asymptomatic individuals 20 years of age to 96% of those 80 years of age, with a large increase in the prevalence through 50 years.[7] This suggests that imaging findings defining degenerative changes are products of normal aging as opposed to pathological processes requiring some form of intervention.
Pathophysiology
Intervertebral disc degeneration is a cellular process, pro-inflammatory process, and molecular process. Aging, genetic disposition, and abnormal mechanical loading all contribute to the acceleration of this process. Disc pain arises from sensitization secondary to the ingrowth of nerve fibers within annular fissures. In a healthy disc, neural penetration through the annulus is about 3 mm. Degenerative discs have shown penetration deeper into the inner third and even nucleus of the disc.[2] Exposure of the nucleus to the outer annulus and neuronal tissue results in the attraction of inflammatory mediators. The result is hyperinnervation and hyperalgesia related to the leakage of pro-inflammatory cytokines. Studies have demonstrated an increase in nerve growth factor in those individuals with discogenic pain.[8] Furthermore, degenerated discs show a greater density of nerve fibers within the respective endplates as compared to healthy endplates.
History and Physical
Patients with discogenic pain will typically report pain in the midline or the immediate paraspinal region with occasional radiation to the flanks or buttocks. Typically, the pain is worsened with axial loading, sitting, or lumbar flexion and relieved with lumbar extension or lying supine. It is also not uncommon for patients to experience associated stiffness. Given the broad differential diagnosis for non-radicular, axial low back pain, and similarity in clinical features, physical exam maneuvers are relatively poor in accurately diagnosing discogenic pain. Therefore, there are no specific physical tests for diagnosis.
Evaluation
As discogenic pain shares clinical features with other etiologies of axial low back pain, further workup ranging from radiographic imaging to interventional procedures is often necessary. As mentioned previously, disc degeneration can be seen on imaging in asymptomatic individuals, and findings positively correlate with age. Therefore, positive findings on imaging must be taken in the context of the patient’s presentation. Conventional radiographic findings include disc-space narrowing, vacuum disc phenomenon due to accumulation of nitrogen in degenerative fissures, endplate sclerosis, and osteophyte formation. CT can identify these same changes earlier in the course of the disease process. MRI is the modality of choice to evaluate disc degeneration due to superior soft-tissue contrast. High-intensity zone (HIZ) is an MRI finding seen on T2-weighted imaging as a hyperintense signal within the posterior annulus that has been shown to correlate with annulus damage as well as pain.
Additional findings are Modic changes, which are degenerative changes in the vertebral endplates and bone marrow. There are three types of Modic changes based on T1-weighted and T2-weighted characteristics. Type I Modic changes are seen as a low signal in the endplates and adjacent marrow on T1-weighted imaging but hyperintense on T2-weighted imaging (See figure). These changes are highly associated with disc degeneration and pain and have high specificity for positive discography.[9]
Provocative discography is a fluoroscopically-guided diagnostic procedure involving deliberate administration of contrast into the nucleus pulposus of the suspected painful disc. The pressurized injection of contrast simulates mechanical loading and induces pain. Additionally, the pattern of contrast spread is indicative of the degree of disc disruption. This procedure is only performed when there is a high pretest probability of discogenic pain based on patient presentation and imaging. This is in part due to potentially significant post-procedural complications, including diskitis, dural puncture, disc rupture from contrast overpressurization, and worsening of underlying disc degeneration. It is difficult to define sensitivity and specificity for the procedure as there is no other gold standard for comparison. Due to variability in technique and interpretation, there is no consensus in regards to the false-positive rate. However, systematic review and meta-analysis suggest a rate of about 9.3% per patient.[10] Given these considerations, the procedure should only be performed if it will make a clear difference in management.
Treatment / Management
As with other causes of axial low back pain, conservative approach with physical therapy and institution of home exercise is the first step in treatment. Regarding pharmacological therapy, NSAIDs may provide moderate efficacy, but long-term use should be monitored due to the impact on the gastrointestinal and genitourinary systems. Regarding opioids in the treatment of chronic back pain, evidence for efficacy is scant in systematic reviews. Additionally, randomized controlled trials are few. Though opioids appear to have short-term efficacy in treating chronic back pain, the improvements in function are unclear [11]. Furthermore, long-term opioid use is associated with well-known effects such as hyperalgesia, tolerance, and potential addiction and overdose. As a result, the CDC has cautioned against the routine use of opioids in the treatment of chronic low back pain. It has recommended that clinicians carefully reassess evidence of risk and benefit when considering an increase to 50 morphine milligram equivalents (MME) or more per day and avoid increasing daily dosage to 90 MME or more.[12]
There are a number of interventional therapies that are used to target discogenic pain that is unresponsive to conservative management. These include epidural steroid injection, nucleoplasty, intradiscal injection, intradiscal electrothermal therapy (IDET), and biacuplasty. Epidural steroid injection has been shown in a systematic review to have fair efficacy in treating discogenic pain.[13] The underlying mechanism, however, is not entirely clear but may involve a corticosteroid-related reduction in pro-inflammatory mediators. IDET and biacuplasty involve the application of heat to destroy sensory fibers innervating the disc. IDET involves the fluoroscopically-guided placement of an active tip near the area of damage. Biacuplasty creates heat across the posterior annulus using a cooled bipolar radiofrequency device. A systematic review by Helm et al. looking at multiple randomized controlled trials involving these intradiscal thermal therapies concluded level I evidence favoring efficacy of biacuplasty in the treatment of discogenic chronic LBP, whereas IDET showed level III (moderate evidence) of efficacy.[14]
Intradiscal injection with glucocorticoid and stem cell solutions are also proposed treatments. A randomized controlled trial performed by Nguyen et al. demonstrated poor long-term efficacy of discogenic pain treated with intradiscal corticosteroid.[15] Intradiscal biological therapy with platelet-rich plasma (PRP) is an emerging treatment option. PRP is an autologous blood concentrate containing growth factors and cytokines. The PRP concentrate is thought to induce tissue regeneration and repair through anabolic and anti-inflammatory effects. Invitro and animal studies have shown the restoration potential of intervertebral discs. However, there is a dearth of double-blind, randomized controlled trials studying intradiscal PRP, though there are other studies that support its safety and analgesic effects.[16] Additionally, the preparation of the concentrates is highly variable. Therefore, more large-scale randomized controlled studies are needed.
Lastly, surgical fusion also is a proposed treatment for patients who have discogenic pain refractory to conservative and minimally invasive treatments. Currently, there is debate regarding the surgical management of discogenic pain with varying results according to different studies.[17] As a substitute for spinal fusion, artificial disc replacement is another more recent therapy intended to help with pain while also preserving the lumbar spine’s function as a motion segment. This may also help prevent adjacent segment disease typically seen post-fusion. Though further studies are currently needed, a recent meta-analysis showed significant improvement in Oswestry Disability Index, satisfaction, and decrease in reoperation rate compared to fusion.[18] Additionally, as the procedure is performed through the abdomen or retroperitoneum, there is theoretically a decreased risk of muscular dissection compared to posterior fusion, which could result in less postoperative pain.
Differential Diagnosis
As discogenic pain is axial, other causes of axial back-pain must be considered. This includes facet arthropathy, paraspinal muscle sprain or strain, ligament sprain or strain, lumbar spondylosis, lumbar spondylolysis, and lumbar spondylolisthesis. Therefore, a detailed history and careful physical exam, along with pertinent imaging, can help to make the correct diagnosis or diagnoses.
Prognosis
Of the patients with chronic low back pain who remain disabled for more than 6 months, less than half return to work. After 2 years, this becomes less likely.[19] For Americans younger than 45 years old, chronic LBP, irrespective of etiology, is the most common cause of disability. Therefore, conservative treatment should begin as soon as possible. Regarding chronic low back pain, poor prognostic factors include emotional distress, ongoing litigation, somatization, and chronic tobacco use.[20][21] Favorable prognostic factors include good social support and symptoms consistent with findings on MRI.
Complications
The complications of discogenic pain include significant disability as well as effects on the psychological well-being of patients. There can be a significant increase in stress, depression, and anxiety after the onset of low back pain. In the setting of very progressive degenerative disc disease, the loss of disc height can result in a decrease of the foraminal diameter, resulting in compression of the nerve root and radiculopathy.
Deterrence and Patient Education
A benefit of having the patient engage in physical therapy early includes patient education in managing and preventing worsening of symptoms. Patients can learn about mechanical loading strategies, provided postural education, a walking program, and receive lumbar taping. The McKenzie Method is a comprehensive approach to chronic low back pain that includes both an assessment and an intervention and incorporates the patient’s directional preference.[22] Depending on the underlying pathology, the patient is provided with specific postures and repetitive movements.
Enhancing Healthcare Team Outcomes
Chronic low back pain, inclusive of discogenic etiology, is an interprofessional problem involving primarily physical therapists, primary care physicians, orthopedists, neurosurgeons, and pain medicine specialists. Interprofessional communication must be encouraged through gathering, lecturing, and sharing of recent updates in treatment. Given the societal and economic burden of this disease, all practitioners have a responsibility to address this issue, given the strains on global healthcare costs.
Furthermore, given the lack of specificity of axial low back pain and often-seen positive imaging in many asymptomatic patients, an emphasis should be made on proper history-taking. This can help prevent unnecessary treatments and risk harm to the patient.
(Click Image to Enlarge)
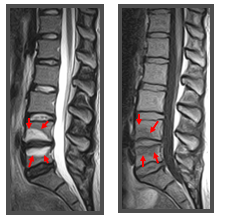
Type 1 Modic changes seen on T2-weighted (left) and T1-weighted (right) MRI highlighting degenerative changes in the vertebral endplates and bone marrow of lumbar vertebral body.
Contibuted by Sanket Pathak