Lumbosacral Radiculopathy
- Article Author:
- Christopher Alexander
- Article Editor:
- Matthew Varacallo
- Updated:
- 7/19/2020 4:35:58 PM
- For CME on this topic:
- Lumbosacral Radiculopathy CME
- PubMed Link:
- Lumbosacral Radiculopathy
Introduction
Low back pain is one of the most common musculoskeletal complaints encountered in clinical practice. It is the leading cause of disability in the developed world and accounts for billions of dollars in healthcare costs annually. Although epidemiological studies vary, the incidence of low back pain is estimated to be anywhere between 5% to more than 30% with a lifetime prevalence of 60% to 90%. Most occurrences of low back pain are self-limited and resolve without intervention. Approximately 50% of cases will resolve within one to two weeks. 90% of cases will resolve in six to 12 weeks. The differential for low back pain is broad, and amongst other diagnoses, should include lumbosacral radiculopathy. Lumbosacral radiculopathy is a term used to describe a pain syndrome caused by compression or irritation of nerve roots in the lower back. It can be caused by lumbar disc herniation, degeneration of the spinal vertebra, and narrowing of the foramen from which the nerves exit the spinal canal. Symptoms include low back pain that radiates into the lower extremities in a dermatomal pattern. Other accompanying symptoms can include numbness, weakness, and loss of reflexes, although the absence of these symptoms does not exclude a diagnosis of lumbosacral radiculopathy. [1]
Etiology
The noxious stimulus of a spinal nerve creates ectopic nerve signals that are perceived as pain, numbness, and tingling along the nerve distribution. Lesions of the intervertebral discs and degenerative disease of the spine are the most common causes of lumbosacral radiculopathy. However, any process that causes irritation of the spinal nerves can cause radicular symptoms. The differential diagnosis for lumbosacral radiculopathy should include (but is not limited to) the following:
- Degenerative conditions of the spine (most common causes)
- Spondylolisthesis: in the degenerative setting, this occurs as a result of a pathologic cascade including intervertebral disc degeneration, ensuing intersegmental instability, and facet joint arthropathy
- Spinal stenosis
- Adult isthmic spondylolisthesis is typically caused by an acquired defect in the par interarticularis
- Pars defects (i.e. spondylolisis) in adults are most often secondary to repetitive microtrauma
- Trauma (e.g. burst fractures with bony fragment retropulsion)
- Clinicians should recognize spinal fractures can occur in younger, healthy patient populations secondary to high-energy injuries (e.g. MVA, fall from height) or secondary low energy injuries and spontaneous fractures in the elderly populations, including any patient with osteoporosis
- Associated hemorrhage from the injury can result in a deteriorating clinical and neurologic exam
- Benign or malignant tumors
- Metastatic tumors (most common)
- Primary tumors
- Ependymoma
- Schwannoma
- Neurofibroma
- Lymphoma
- Lipomas
- Paraganglioma
- Ganglioneuroma
- Osteoblastoma
- Infection
- Osteodiscitis
- Osteomyelitis
- Epidural abscess
- Fungal infections (e.g. Tuberculosis)
- Other infections: lyme disease, HIV/AIDS-defining ilnesses, Herpes zoster (HZ)
- Vascular conditions
- Hemangioblastoma, aterior-venous malformations (AVM)[2]
Epidemiology
While the literature lacks concise epidemiologic data, most reports estimate about a 3% to 5% prevalence rate of lumbosacral radiculopathy in patient populations. Moreover, the condition constitutes a significant reason for patient referral to either neurologists, neurosurgeons, or orthopedic spine surgeons.
While the incidence of low back pain is estimated to be between 13% and 31%, the incidence of radicular symptoms in patients presenting with low back pain ranges from 12% to 40%. In the workforce, low back pain is the second greatest cause of absenteeism behind upper respiratory tract infections. About 25 million people miss one or more days of work due to low back pain, and more than five million are disabled from it. Patients with chronic back pain account for 80% to 90% of all health care expenditures. [1][3]
Pathophysiology
Lumbosacral radiculopathy is the clinical term used to describe a predictable constellation of symptoms occurring secondary to mechanical and/or inflammatory cycles compromising at least one of the lumbosacral nerve roots. Patients can present with radiating pain, numbness/tingling, weakness, and gait abnormalities across a spectrum of severity. Depending on the nerve root(s) affected, patients can present with these symptoms in predictable patterns affecting the corresponding dermatome or myotome. [4]
History and Physical
As with any disease process, a thorough history and physical exam are crucial in diagnosing lumbosacral radiculopathy. Pain is the most commonly reported symptom. However, numbness or weakness along the distribution supplied by the respective nerve root(s) is often appreciated. Radicular pain is typically characterized by patients as "electrical shocks" or "shooting pains" that radiate from the buttock to the foot. While gathering the history, it is important to screen for any red-flag symptoms, which could indicate an urgent/emergent clinical condition. Evaluating clinicians must first rule out associated "red flag" symptoms including:
- Thoracic pain
- Fever/unexplained weight loss
- Night sweats
- Bowel or bladder dysfunction
- Malignancy (document/record any previous surgeries, chemo/radiation, recent scans and bloodwork, and history of metastatic disease)
- Can be seen in association with pain at night, pain at rest, unexplained weight loss, or night sweats
- Significant medical comorbidities
- Neurologic deficit or serial exam deterioration
- Gait ataxia
- Saddle anesthesia
- Age of onset (bimodal -- Age < 20 years or Age > 55 years)
A full neurologic exam shoulder is performed, including an assessment for upper motor neuron findings (Babinski sign, clonus, spasticity). On physical exam, several maneuvers can assist the clinician in making a diagnosis. Lasègue test, or straight leg test, is performed by passively raising one leg into the air. This creates increased tension on the sciatic nerve between 30 degrees to 60 degrees from the exam table. A reproduction of the patient's symptoms during passive movement between 30 degrees to 60 degrees is considered a positive sign and is suggestive of lower lumbar nerve root involvement (L4 to S1). Of note, a similar stretch can be created on the femoral nerve using a reverse straight leg, or Ely test. With this test, the patient's symptoms are reproduced by extending the hip and flexing the knee with the patient in the prone position. This will stretch the femoral nerve and the L2 to L4 nerve roots. Reproduction of radicular symptoms can also be produced by placing the patient in a seated position with the neck in full flexion and knees in full extension (slump test). [5][6]
Evaluation
Given the favorable outcome, and often spontaneous resolution of the vast majority of low back pain symptoms, extensive imaging is usually not necessary in patients with low back pain of less than four to six weeks duration. As stated above, work-up begins with a thorough physical exam. Neurologic deficits in a focal distribution warrant further workup. In cases of low back pain that fails to resolve within one to two months, MRI is considered the gold standard in evaluating radicular low back pain. Of note, MRI with contrast is recommended in patients with previous spinal surgeries. For patients unable to undergo MRI, CT scan is an alternative option. However, CT is not as sensitive in visualizing soft tissue or tumors and is not recommended for routine use. X-rays are simple, readily available in most developed countries, and can reveal gross bony abnormalities such as fractures, disc space narrowing, and other osteodegenerative changes. Often, it is not clinically possible to distinguish lumbosacral radiculopathy from peripheral neuropathy or plexopathy. In these instances, electromyography and nerve conduction study can be utilized to localize a lesion with relatively high diagnostic specificity. [7]
Treatment / Management
Treatment is varied depending on the etiology and severity of symptoms. However, conservative management of symptoms is generally considered first line. Medications are used to manage pain symptoms including NSAIDS, acetaminophen, and in severe cases, opiates. Radicular symptoms are often treated with neuroleptic agents. Systemic steroids are often prescribed for acute low back pain, although there is limited evidence to support its use. Nonpharmacologic interventions are often utilized as well. Physical therapy, acupuncture, chiropractic manipulation, and traction are all commonly used in the treatment of lumbosacral radiculopathy. Of note, the data supporting the use of these treatment modalities is equivocal. Interventional techniques are also commonly used and include epidural steroid injections and percutaneous disc decompression. In refractory cases, surgical decompression and spinal fusion can be performed. [8][9][10]
Differential Diagnosis
- Ankylosing spondylitis
- Epidural abscess
- Inflammatory arthritis
- Inflammatory bowel disease
- Leukaemia
- Lumbosacral disc injuries
- Lymphoma
- Metastatic carcinoma
- Multiple myeloma
Pearls and Other Issues
Overall, lumbosacral radiculopathy is an extraordinarily common complaint seen in clinical practice and comprises a large proportion of annual doctor visits. The vast majority of cases are benign and will resolve spontaneously, and thus, conservative management is the most appropriate first step in the absence of clinical red flag symptoms. In cases where symptoms fail to resolve, imaging studies, electromyography, and nerve conduction studies can assist in making a diagnosis. [2][4][10]
Enhancing Healthcare Team Outcomes
Lumbosacral radiculopathy is a common problem and nurse practitioners, physician assistants, and physicians working as a team should be aware of the red flag symptoms that require emergent intervention and reporting to the physician providing team management.
(Click Image to Enlarge)
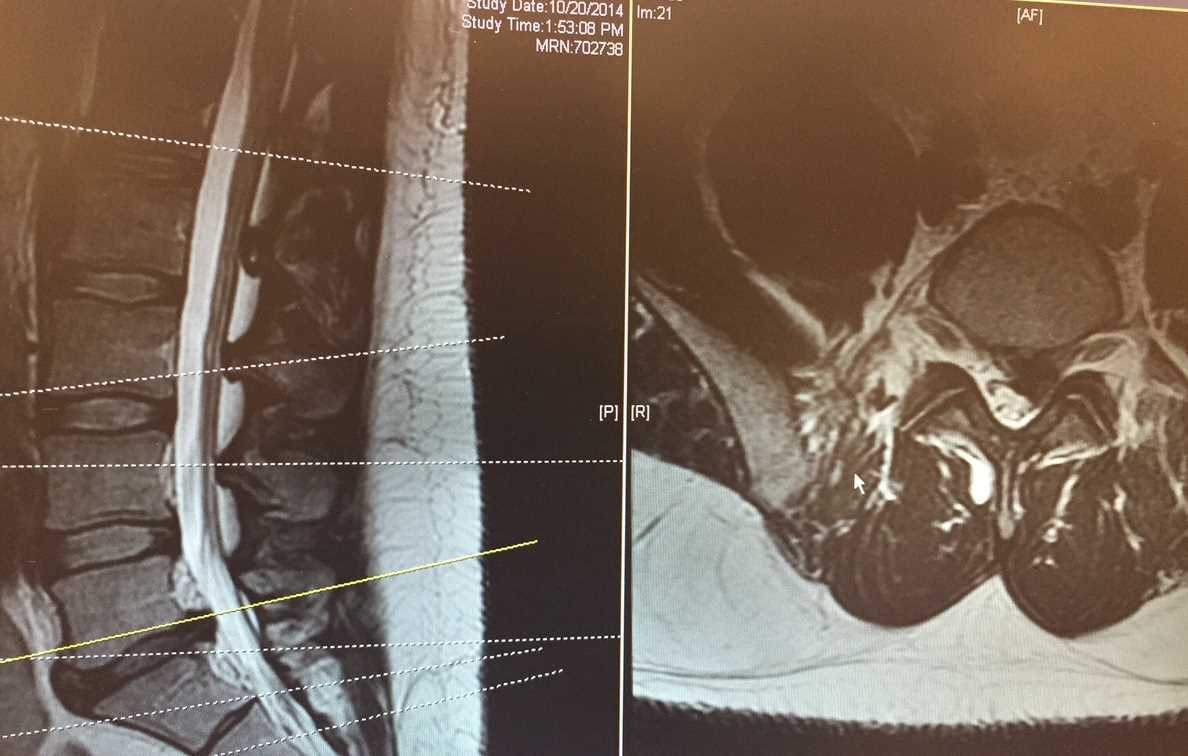
Lumbar MRI T2 sagital and axial slice
Contributed by S. Dulebohn, M.D.