M-plasty
- Article Author:
- Joseph Prohaska
- Article Author:
- Miguel Sequeira Campos
- Article Editor:
- Jonathan Crane
- Updated:
- 10/27/2020 8:02:18 PM
- For CME on this topic:
- M-plasty CME
- PubMed Link:
- M-plasty
Introduction
An M-plasty is an excisional technique used to remove standing cutaneous deformities, also known as dog ears, from the end of a linear repair. Dog ears represent excess tissue formed in the process of wound closure. There are many different techniques for the removal of a dog ear. Non-excisional techniques include serially halving the incision which effectively distributes tissue across the length of the incision. Serially halving may not work in all situations and is dependent on the amount of excess tissue and the length of the wound. For example, this technique will have a limited effect on short incisions or large dog ears. The most common excisional technique for the removal of a dog ear is to remove the excess tissue. A triangular piece of tissue, known as a Burrow’s triangle can be removed anywhere along the length of the incision. Typically, Burrow’s triangles are taken at the end of the incision which will increase the final length of the incision [1]. An M-plasty is an alternative to these standard techniques and has the additional benefit of shortening the final wound length and conserving normal tissue. In some instances, an M-plasty may be used on each end of an incision to shorten the length of the final defect further.
Indications
An M-plasty is a very useful technique used to shorten the expected final wound length of an excision[2][3]. This can be beneficial when longer incisions would be contraindicated, for example, as crossing cosmetic boundaries or extending into sensitive structures. Furthermore, an M-plasty can be used near the lateral canthus to remove a dog ear without disrupting the lateral canthus. This is also an ideal location for an M-plasty because the scar can be concealed within the crow’s feet. Also, an M-plasty may be used to remove dog ears created by flaps. M-plasties can be added to either or both ends of an incision to shorten a wound at the discretion of the surgeon. Although M-plasties do decrease the length of a scar, they increase the width of the scar. This means that M-plasties create a shorter but wider scar. In some cases, this may be cosmetically less noticeable than long incisional lines. For example, large tumors on the back may be less noticeable with an M-plasty on each end compared to a longer, linear repair. The main goal of the M-plasty is to take an excision that would extend across a cosmetic unit and keep it within that cosmetic unit. This helps avoid crossing lines like the jawline.
Contraindications
It is important to note that an M-plasty does not alter tension vectors. Therefore, the contraindications for an M-plasty are the same contraindications for primary closures. Primary wound closure is contraindicated when there is excessive tension on the wound. Excess tension can lead to dehiscence or necrosis of the wound edges. Increased tension can also lead to poor cosmetic outcomes, such as wide, fish-mouth-like scars. More importantly, excessive tension can cause anatomic distortion of sensitive structures such as the eyelid, eyebrow, or mouth.
Equipment
No special equipment, except for a standard surgical tray used for simple skin excisions, is needed for this procedure.
Personnel
This procedure can be performed by the surgeon alone. However, an assistant can be quite helpful and aids in the efficiency of the procedure.
Preparation
Cutaneous surgery can be performed in an office setting. Sterile or nonsterile gloves may be used at the preference of the surgeon as there is not an increased risk of surgical site infections. The skin is prepped with an antiseptic based on the site of surgery and the preference of the surgeon[4][5].
Patient Counseling
The surgeon should counsel the patient about the risks of the procedure, namely infection, bleeding, and the likelihood of recurrence. The procedure should also be thoroughly explained to the patient. This explanation can be aided by visual aids such as a picture of the tumor with the planned excision drawn out. Visual aids can also be used to show the patient how the closure with look after the excision is performed.
Technique
An M-plasty may be designed before excision or later in the repair process. An M-plasty can be best visualized by first drawing out an elliptical incision. To add an M-plasty to one end of the ellipse, the peak of the ellipse is inverted or folded inward on itself to create an “M” (see figure). Overexaggeration of this folding will result in impingement of the margins of the tumor and the incomplete removal of the margins. It is advisable to draw out the margins around the tumor first and then overlay the planned M-plasty. The skin is incised and extirpated in the standard fashion. Undermining is performed in the appropriate plane depending on the body location. The final configuration of an M-plasty is a “Y,” with the base representing the linear closure and the arms of the “Y” representing the M-plasty. Sutures can be placed in either running or interrupted fashion. The tip of the M-plasty may benefit from the placement of a tip stitch to properly align the tissue. If an M-Plasty is done prior to the removal of a malignancy, it is important to confirm that the tip of the M-plasty does not extend into the margins of the malignancy[3][6].
If an M-plasty is used to remove a dog ear, the dog ear is elevated with forceps then 2 incisions are made at 45-degree angles on either side of the dog ear and burrows triangles are removed. This essentially creates the “Y” shaped closure. The excess tissue is removed from the lateral sides of the incision, sparing the “V” created by the 2 incisions. The wound is then repaired in the same fashion as above.
Nested M-Plasty
A nested M-plasty is a variant of a traditional M-plasty and can be described as an M-plasty within an M-plasty. If a regular M-plasty shortens the length of the scar and preserves healthy tissue, then doing the process twice can produce even shorter scars and preserve even more tissue. A standard M-plasty can be visualized as an ellipse with the peak of the ellipse folded inward. This produces 2 side-by-side triangles that are half the size of the ellipse. A nested M-plasty repeats this process. Each of the triangles is folded in itself again creating four side-by-side triangles that are one-quarter the size of the ellipse (see figure). A tip stitch as with a regular M-plasty can be quite useful for this type of closure. This technique is best used for flat or concave surfaces as it can induce bunching of the skin, which typically flattens out with time. Bunching of skin over convex surfaces can be quite noticeable and tends to persist[7].
Clinical Significance
M-plasties are a tissue-sparing alternative for the removal of dog ears and should be in every cutaneous surgeon’s repertoire.
Enhancing Healthcare Team Outcomes
M-plasty is usually performed by a plastic or cosmetic surgeon. Clinicians including nurses who have patients with incisions like dog ears should be referred to a plastic surgeon. The procedure should not be performed by someone who has no experience of scar revision.
(Click Image to Enlarge)

Nested M-plasty. Note the duplication of the M-plasty technique.
Illustrated by Tony Burbatt. Personal permission received.
(Click Image to Enlarge)
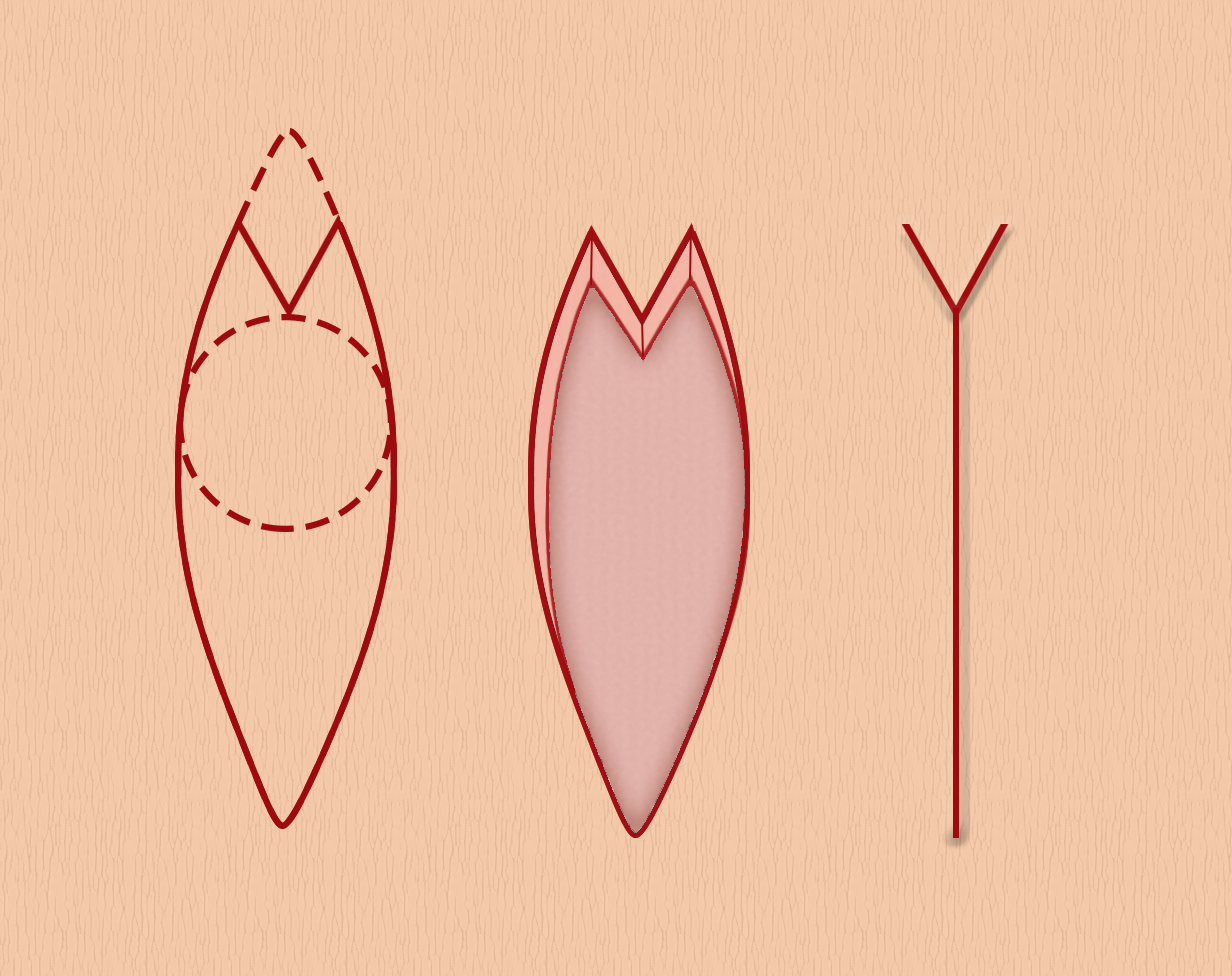
Figure 1. Stages of an M-plasty. The image on the left represents the planning stage of an M-plasty. The middle image illustrates the wound post excision and the image on the right illustrates the appearance of the wound after closure.
Illustration courtesy of Anthony Burbatt. Reprinted with permission.
(Click Image to Enlarge)
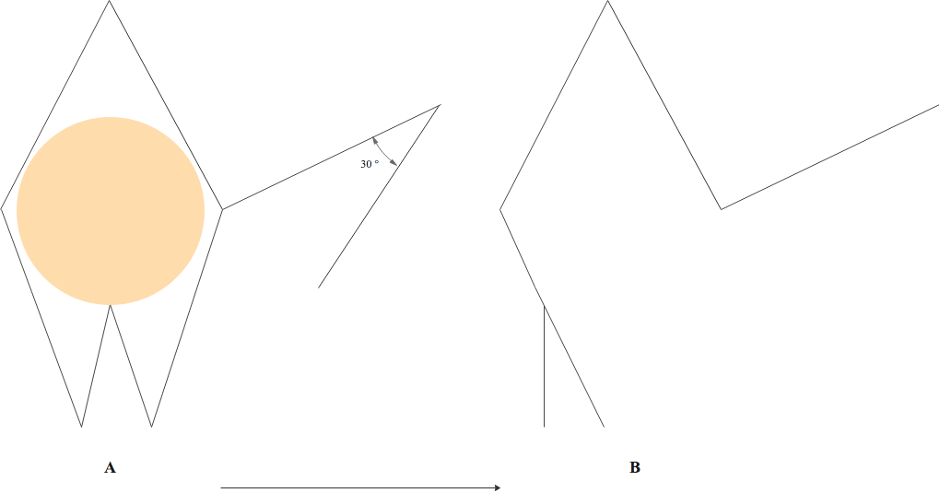
Figure 3: Webster Rhombic Flap Modification. A 30-degree flap tip angle combined with M-plasty to close the defect base. A: defect (orange) extended into modified rhomboid shape and with 30-degree flap. B: wound closure lines following flap transposition, M-plasty closure of defect base and closure of donor site.
Contributed by Elizabeth Wilkinson/ Peter Macneal, MBChB Design based on original journal article: Webster R, Davidson T, Smith R. The thirty degree transposition flap. Laryngoscope. 1978;88.(1):85–94