Morton Neuroma
- Article Author:
- Usama Munir
- Article Author:
- Dawood Tafti
- Article Editor:
- Samer Morgan
- Updated:
- 6/2/2020 8:17:00 PM
- For CME on this topic:
- Morton Neuroma CME
- PubMed Link:
- Morton Neuroma
Introduction
Morton’s neuroma is a compressive neuropathy of the forefoot interdigital nerve. Neuropathy is chiefly due to compression and irritation at the plantar aspect of the transverse intermetatarsal ligament. It is not a true neuroma as the condition is degenerative rather than neoplastic. It is also referred to as Morton’s metatarsalgia, interdigital neuritis, Morton’s entrapment, interdigital neuralgia, interdigital neuroma, interdigital nerve compression syndrome, and intermetatarsal neuroma. The most common location for a Morton's neuroma is between the 2nd and 3rd metatarsals.[1][2][3]
Etiology
Interdigital neuromas occur as a result of compression of the interdigital nerve against the distal end of the transverse metatarsal ligament during dorsiflexion of the toes. Common causes include narrow toe-box footwear, hyperextension of the toes in high-heeled shoes, deviation of the toes, inflammation of the intermetatarsal bursa, thickening of the transverse metatarsal ligament, forefoot trauma, high impact sporting activities, metatarsophalangeal joint pathology, and lipoma.[4][5]
Epidemiology
Pathophysiology
Morton’s neuroma is common in the third interspace because it is narrower compared to other spaces. As the common digital nerve to the third space receives branches from both medial and lateral plantar nerves, it has increased thickness and is prone to compression and trauma. Trauma from a crush injury, penetrating injury, thickened transverse metatarsal ligament, enlarged bursa in the interspace, and repetitive trauma from running have all been linked to the development of Morton’s neuroma. The compression and repetitive trauma to the nerve results in vascular changes, endoneurial edema, and excessive bursal thickening leading to perineural fibrosis.[8]
Histopathology
Grossly there is a fusiform swelling near the bifurcation of plantar interdigital nerve with thickening of adjacent tenosynovial tissues. Microscopically there is endarterial thickening of the digital artery, usually with thrombosis, fibrosis surrounding and within the nerves, Schwann cell and fibroblast propagation, and damage of myelinated nerve fibers.
History and Physical
The most common symptoms are plantar pain between metatarsal heads that are aggravated by walking and wearing tight-fitting, high-heeled shoes and relieved by resting and removing shoes. Patients describe the pain as burning, stabbing, or tingling with electric sensations. Some patients describe the sensation as walking on a stone or marble. Numbness between the toes is present in less than half of the patients. With prolonged walking, the pain can radiate to the hindfoot or leg causing cramps.
Evaluation
Diagnosis is usually based on history and clinical examination. Palpation in the affected space may reproduce the symptoms. Compression of the forefoot in the mediolateral direction while palpating the affected space often results in a significant crunching or clicking feeling, commonly known as the "Mulder’s click." Some surgeons inject the affected webbed space with a diagnostic injection of lidocaine. A maximum of 1 ml to 2 ml of the anesthetic agent should be injected. Plain, weight-bearing radiographs should be taken to rule out any bony masses, deformities, subluxation, dislocation, or arthritis. A radio-opaque foreign body can also be visualized. Ultrasound scan performed by an experienced radiologist can be a useful diagnostic aid. A steroid injection under ultrasound guidance can be given at the same time. MRI can potentially be obtained based on the clinical scenario, especially to rule out other pathologies.[5][9]
When obtained, MRI imaging demonstrates a dumbell shaped soft tissue lesion within the intermetatarsal space. T1 signal is often low, T2 signal is frequently low or intermediate, and enhancement is variable. Sonographic evaluation also similarly demonstrates a noncompressible dumbell shaped soft tissue lesion with hypoechogenicity within the intermetatarsal space. A "Mulder’s click" can potentially be elicited on palpation with the probe.
Treatment / Management
Nonoperative Treatment
Wearing a wide, soft-soled, laced shoe with a low heel can be effective in relieving pressure on the nerve. Some surgeons recommend a firm-soled shoe instead. A soft metatarsal support can help to spread the metatarsal heads. In the presence of synovitis, instability or deformity of the toe, a Budin splint or canopy toe strapping can decrease secondary neuralgia. Anti-inflammatory medications, tricyclic antidepressants such as amitriptyline, and anti-seizure medications such as gabapentin can potentially be administered to lessen the severity of related nerve symptoms. Blind or ultrasound-guided steroid injections can occasionally help, but their effect is rarely long-lasting. Atrophy of the subcutaneous fat and plantar fat pad, discoloration of skin and disruption of the joint capsule adjacent to the injected site causing deformity of the toe are some of the reported side effects. Radiofrequency ablation, cryotherapy, and alcohol nerve injections have been proposed as a less invasive and more conservative method of treating neuromas.[1][10][11]
Surgical Treatment
If non-operative management fails, then surgery is indicated to treat recalcitrant cases. The neuroma is excised using a dorsal or plantar approach. The dorsal approach is better tolerated by patients as the plantar scar can itself be painful. A 3 cm to 4 cm incision is made just proximal to the involved webspace in the midline to prevent injury to the dorsal cutaneous nerves. The incision is deepened to the transverse metatarsal ligament which is transected. The common digital nerve is identified in the proximal portion of the wound and is traced distally to its bifurcation. Proximally, the common digital nerve is cut proximal to the metatarsal heads and is then traced distally past the bifurcation where both the branches are transected. Some surgeons suture the cut ends of the nerve to the side of the metatarsal or one of the intrinsic muscles to prevent the formation of a painful stump neuroma. As little plantar fat as possible should be removed. A postoperative shoe is worn till the stitches are removed at about 7 to 14 days, and a compressive wrap is used for 2 to 6 weeks.
The plantar incision is mainly reserved for recurrent neuromas or when the patient has a very proximal focal tender trigger point for the neuralgia. It decreases the rate of missed neuroma, and it does not require an incision of the transverse metatarsal ligament. The plantar approach permits a more direct exposure of the nerve and allows its more proximal resection. The artery and vein can be better visualized and preserved. The main disadvantages are painful plantar scars and plantar keratosis in about 5% cases.[12]
Differential Diagnosis
- Metatarsal stress fracture
- Hammer toe
- Rheumatoid or osteoarthritis
- Malignancy
- Ganglion cyst
Prognosis
Conservative Approaches
Conservative approaches to treatment have shown varying degrees of effectiveness. [13] [14] Change of footwear, activity modification and pharmacotherapy are often used to minimize pain and lessen symptoms. Employing multiple strategies has shown to be effective. [15]
Surgical Cases
Various papers have investigated success rates after surgery. [16] [17] [18] [19] Kasparek et al. evaluated 81 patients and noted excellent subjective results in 45% of patients and a good result in 32% of patients. Approximately 8% of patients had noted a poor result. [16]
Complications
- Chronic pain
- Complications related to surgery
- Complications associated with corticosteroid injections
Deterrence and Patient Education
Managing patient expectations is key. The patient should be educated about the variable success rates of physiotherapy, activity modification, using appropriate footwear, and the role of other modalities such as injections and cryotherapy. When surgery is being considered, a significant minority of patients report worsening of pain after surgery. [15] [16]
Pearls and Other Issues
If there has been inadequate proximal resection or failure of the nerve to retract, the neural stump can become enlarged and bulbous. The neural stump may also adhere to adjacent bone and soft tissue, causing traction neuritis. It can cause pain and tenderness in the webbed space of previous neuroma excision at or proximal to metatarsal heads. The clinical examination, investigations and non-operative management are same as for a primary neuroma. For surgery, both dorsal and plantar incisions are recommended. The dorsal incision has to be extended proximally to visualize the stump, but sometimes, exposure can be difficult. The plantar approach is considered to provide a better exposure so that the nerve is identified and resected easily.
Enhancing Healthcare Team Outcomes
Morton neuroma is best managed non-surgically with a team of healthcare professionals that includes a podiatrist, orthopedic surgeon, sports physician, nurse practitioner, and primary care provider. The patient may require pain medications, but the key is changes in shoe wear. The nurse should encourage the patient to wear appropriate non-constrictive shoewear that is well padded. Obese patients may benefit from weight loss, and hence a dietary consult is appropriate. The patient may benefit from physical therapy, use of warm compress and ice to ease the pain. [20][21](Level V)
Outcomes
The majority of patients with Morton's neuroma have a good recovery with non-surgical treatment. A few patients may require surgery if the neuroma is localized and can be excised. However, even after surgery, the recurrence rate neuroma and/or pain are very high. The key is to change footwear and lose weight. [22][23](Level V)
(Click Image to Enlarge)

Morton neuroma
Image courtesy S Bhimji MD
(Click Image to Enlarge)
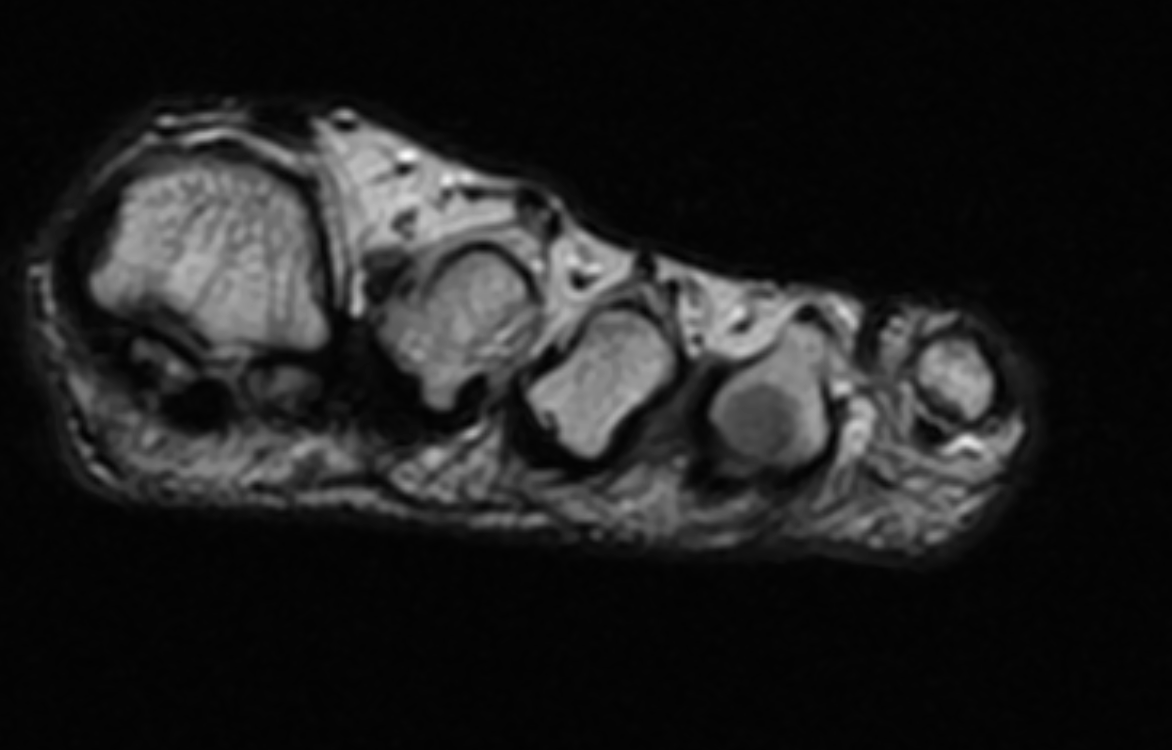
Coronal T1 image demonstrates a low signal lesion between the third and fourth metatarsals consistent with a Morton's neuroma.
Contributed by Dr.Dawood Tafti, MD.
(Click Image to Enlarge)

Coronal T1 MRI image demonstrates a Morton's neuroma between the third and fourth metatarsals.
Contributed by Dawood Tafti, MD.