Nasopharyngeal Carcinoma
- Article Author:
- Abdul Basit Shah
- Article Author:
- Hassam Zulfiqar
- Article Editor:
- Shivaraj Nagalli
- Updated:
- 9/8/2020 8:47:26 AM
- For CME on this topic:
- Nasopharyngeal Carcinoma CME
- PubMed Link:
- Nasopharyngeal Carcinoma
Introduction
Nasopharyngeal carcinoma (NPC), previously known as lymphoepithelioma, is a malignancy arising from the epithelium of the nasopharynx. Endemic to China, the malignancy shows a variable rate of occurrence ranging from high incidence in the Southern part of China to a low rate in the White population and Northern China with the incidence ranging from 15 to 50 per 100000. A complex interplay of genetic susceptibility and Epstein Barr virus (EBV) infection is responsible for the disease.[1]
Etiology
An interplay of environmental factors, genetic structure, and EBV infection is involved in the etiology of the disease. Environmental factors, including smoking in the western population and nitrosamines containing food agents, have been considered to have an involvement. Secondly, the genetic structure of the demographics involved also plays a vital role, as explained by the overwhelming incidence in the Chinese population. Lastly, EBV infection, coupled with genetic susceptibility, has shown a substantial relevance to the disease.[2][3]
Epidemiology
Nasopharyngeal carcinoma (NPC) is highly endemic to Southern China, Malay and Indonesian population along with people from Southeast Asia. The rate varies from a minuscule value of less than 1 per 100000 individuals in non-endemic areas to a high value of 25 to 30 and 15 to 20 males and females per 100000 individuals in endemic areas, respectively.[4]
Histopathology
Histopathological evaluation can elucidate in which category does the tumor fall. On histopathological grounds, NPC can fall into three main sub-groups as per WHO classification[5]:
- Keratinizing type (20% to 25%)
- Non-keratinizing differentiated type (10% to 15%)
- Non-keratinizing undifferentiated (60% to 65%)
History and Physical
Patients can have variable presentations depending on the area of involvement of the disease.
- Nasal symptoms: A subset of patients present with nasal symptoms ranging from nasal obstruction, blood-tinged nasal discharge, and post-nasal drip to denasalization of voice and cacosmia. Symptomatology is proportionate to the size of growth and the extent of local involvement. Around 80% of the individuals suffering from the disease present with nasal symptoms
- Otological symptoms: Patients present with symptoms secondary to eustachian tube blockage, i.e., conductive hearing loss, effusions and fullness, and tinnitus. Half of the patients with NPC have some form of otological complaint during the disease caused because of the growing mass obstructing the outflow of the eustachian tube.
- Neurological symptoms: Intracranial extension is prevalent among 8% to 12% of the demographic — various forms of cranial nerve involvement present with the associated symptom. The most commonly involved nerve is the abducens nerve.[6]
- Nodal involvement: One of the most common presenting features would be an enlarged neck node. Lymph nodes of the apex of the posterior triangle and the upper jugular are most commonly involved initially. Supraclavicular nodes are the last to be involved and are a sign of advanced disease.[7]
Distant metastasis and paraneoplastic syndrome: Symptoms associated with distant spread rarely present to the primary caregiver. The most significant spread includes the liver and lungs. It is sometimes difficult to assess the primary site of malignancy when metastatic pulmonary lesions occur. PET scan aids in the differentiation of the two. Secondly, a handful of cases present with symptoms of dermatomyositis. The progression of the disease might initiate with the malignant lesion or can present after the initial diagnosis of NPC.[8]
Evaluation
Lab Investigations
- Baseline investigations which include complete blood count, renal and liver function tests can be sent for initial scrutiny. An abnormality would be detected in cases where a hepatic extension is suspected along with a deterioration in renal function as the tumor divides at a rapid pace.
- Epstein Barr virus invariably has involvement in the pathogenesis of the disease process. To establish an association, serum IgA levels are necessary. These carry both diagnostic and prognostic significance for the disease process.[8]
Imaging Studies
- CT scan: A local tumor is visible, extending from the roof of the pharynx. CT scan is the modality of choice as far as bone invasion, and intracranial extension is also present. However, radiation exposure and its limited value in terms of soft tissue extension and nodal metastasis make MRI the preferred modality.
- MRI scan: MRI is the superior modality for assessing the tumor extension into the musculature and the nodal metastasis. The tumor bulk, along with local invasion, can be easily visualized and does not pose any threat of radiation.
- PET scan: It is the modality of choice for assessing remission and for investigating recurrence. PET-CT scan can augment the extent of distant metastasis as it is a whole-body scan. However, MRI can provide a higher level of local delineation, making it still the investigation of choice for local spread.[9]
Endoscopic Evaluation and Histopathological Analysis
- The tumor is visible via nasopharyngoscopy, and the local extension along with tumor size is assessable, and biopsy possible. However, the assessment becomes hindered if the mass is too large for accessing the passage.
Treatment / Management
The mainstay of treatment for NPC is radiotherapy in locoregional lesions as the non-keratinizing variety is highly radiosensitive. Surgical intervention is limited to salvage procedures in recurrent diseases, whereas chemotherapy is preferred concomitantly with radiation in advance stages.
Radiotherapy
Radiation is the management of choice for the loco-regional lesion. Radiotherapy is effective in all cases except those for distant metastasis hence from stage I to stage IVB. NPC shows a tendency for quick spread regionally, especially as the nasopharynx is a small cavity so spread to paranasopharyngeal spaces, musculature, and nodes common. Also, progressively involving the contralateral side is not a rare occurrence. Consequently, a dose of approximately 65 Gy for primary tumor with 50 to 55 Gy is also necessary for nodal negative necks.
A recent innovation in the delivery system employed for radiation is intensity modulation or intensity-modulated radiotherapy (IMRT). The system comes equipped with a CT taking slices of the area involved. The physician specifies the targeted area of the beam and modulates the intensity of the beam employed.[10]
Brachytherapy is another innovative technique for targeted radiotherapy. The technique used is the implantation of gold grains or iridium implants, jacketed for localized radiotherapy, via a split incision of the soft palate. The technique is useful for localized tumor bulk that has not shown any intracranial extension. The technique spares any local vital organ damage.
Radiotherapy is also employed when treatment failure or recurrence occurs. It has been proven useful in both local recurrence and nodal failures. In such cases, brachytherapy is considered keeping in mind the friability of the local tissue, the general condition of the patient, and the impact on vital organs of the region.[3][9]
Chemotherapy
NPC is highly sensitive to radiation and chemotherapy. In locally advanced regional disease, concomitant chemoradiotherapy is the mainstay of management. The disease responds better with induction, and concurrent therapy is significant in shrinking the tumor bulk. The most frequently used agent as the initial line of chemotherapeutic intervention is Cisplatin. The standard of care is a dose of 100 mg every third week.
Chemotherapy is also the option of choice when distant metastasis is involved. NPC with distant poly-metastasis is offered palliative chemotherapy. The agents of choice are cisplatin and 5-fluorouracil. With recent advances, several chemotherapeutic agents are available for the continuation of therapy. However, the median survival rate is not more than a year.[3][9]
Surgical Intervention
Surgical intervention is employed only as a salvage option. The nasopharynx is a small and deep area that is hard to access, thus making the surgical approach to it sometimes difficult and inappropriate. However, when encoutnering locally recurring disease, patients should be given the option of surgical intervention. Surgery is also one of the key modes of management for distant oligo-metastasis in conjunction with radiotherapy and radio ablation.[11][12]
Nasopharyngectomies are carried out by several approaches, and the approach decided should be tailored in accordance with the expertise of the surgeon and the general condition of the patient. The following are some of the popular approaches to the cavity.
- Inferior approach- via transpalatal incision
- Lateral approach- via the lateral skull base
- Inferolateral approach
- Midfacial degloving
- Endoscopic approach
Radical neck dissections often accompany the procedures mentioned above, where extensive neck involvement is present. Also, in recurring disease, especially nodal recurrence, radical neck dissection is done as a component of salvage therapy.
Differential Diagnosis
Differential diagnosis of NPC depends on regional lesions involving the nasopharynx and mimicking the symptomatology. Categorization is possible regarding the nature of the lesion as follows:
Benign conditions
- Nasopharyngeal polyposis
- Angiofibromas
Malignant lesions
- Lymphomas,
- Salivary gland tumors
- Sinonasal carcinomas
- Malignant mucosal melanomas
Staging
The nuances in imaging techniques and the improved outcomes associated with optimum therapy have caused the American Joint Committee on Cancer (AJCC) to reevaluate the staging process. As per the recent guidelines, the TNM staging has been explained as per the following criteria[13]:
Primary Tumor (T):
- Tx: Inability to assess the tumor.
- T1: Nasopharyngeal involvement sparing the parapharyngeal spaces
- T2: Extension into the parapharyngeal spaces and may or may not extend into regional muscles(Pterygoids and prevertebral)
- T3: Invasion of skull and sinuses
- T4: Intracranial extension with the involvement of Cranial nerves, pterygoids, and orbit.
Nodal metastasis (N):
- NX: Inability to assess nodal involvement
- N0: No involvement
- N1: A unilateral spread not exceeding 6 cm in maximum dimensions confined above supraclavicular fossa
- N2: A bilateral spread not exceeding 6 cm in maximum dimensions confined above supraclavicular fossa
- N3: Metastasis
- N3a: involvement greater than 6 cm
- N3b: supraclavicular fossa involvement
Distant Metastasis (M):
- MX: Inability to assess metastasis
- M0: No distant involvement
- M1: Distant Involvement.
Stage grouping:
- Stage 0: T1s-N0-M0
- Stage I: T1-N0-M0
- Stage II: T1-N1-M0 and T2-N0-M0
- Stage III: T1, T2-N2-M0 and T3-N0, N1, N2-M0
- Stage IVA: T4-N0, N1, N2-M0
- Stage IVB: Any T-N3-M0
- Stage IVC: Any T-Any N-M1
Prognosis
The overall prognosis and the 5-year survival rate has improved since the advent of nuances in the radiotherapy techniques. This change shows a drastically decreased the mortality and morbidity associated with illness from a reported 5-year survival of 25% to 40% to approximately 70% in the past decade.[14]
Complications
Lesions can have local complications, including obstruction of Eustachian tubes causing otitis media with effusion (OME), persistent nasal obstruction, and obstruction of the oropharyngeal airway. Mass effect causing blockage of oropharynx impedes swallowing, and if it remains unchecked, its progression may lead to blockage of the airway. Intracranial extension and involvement of cranial nerves are debilitating and can have a lifelong disability even after management.[15]
Deterrence and Patient Education
Patients endemic to prevalent areas should be more vigilant regarding the symptoms of the disease. Moreover, the demographics of the western population having environmental factors (smoking, etc.) associated with NPC should also receive education regarding their hazardous effects. Also, the subset of people having genetic susceptibility along with recurrent EBV infection should have a higher index of suspicion for the disease.
Pearls and Other Issues
- NPC is a malignancy having a variable incidence depending on the region.
- Endoscopic biopsy should be the first and foremost step for the evaluation of the lesion.
- NPC has a high index of susceptibility to radiotherapy; hence should be considered in almost all forms of the disease at the initial presentation. Coupling the effectiveness of this mode of management with difficulty associated with the surgical approach to the region makes radiotherapy the therapy of choice.
- In advance cases, chemotherapy is given concomitantly to produce optimum results. The drug of choice is cisplatin initially, given concomitantly with radiotherapy.
Enhancing Healthcare Team Outcomes
Endemic areas have made strides in this regard as they have increased their index of suspicion towards such malignancies at the primary care physician level. NPC requires the efforts of an interprofessional team.
After diagnosis, a radiotherapist and oncologist should educate the patient regarding the favorable outcome associated with strict adherence to the program. Otolaryngology and otolaryngology nurses provide care and education to these patients. Board-certified oncologic pharmacists review prescriptions and check for drug-drug interactions. Oncology specialty nursing staff can administer chemotherapy, assist in post-procedural care and monitoring, and report any concerns to the treating clinicians. Prolonged therapy has complications of itself that are manageable in follow-up clinics. Also, patients having the psychological burden, benefit from structured support groups and psychologist sessions. [Level 5]
(Click Image to Enlarge)
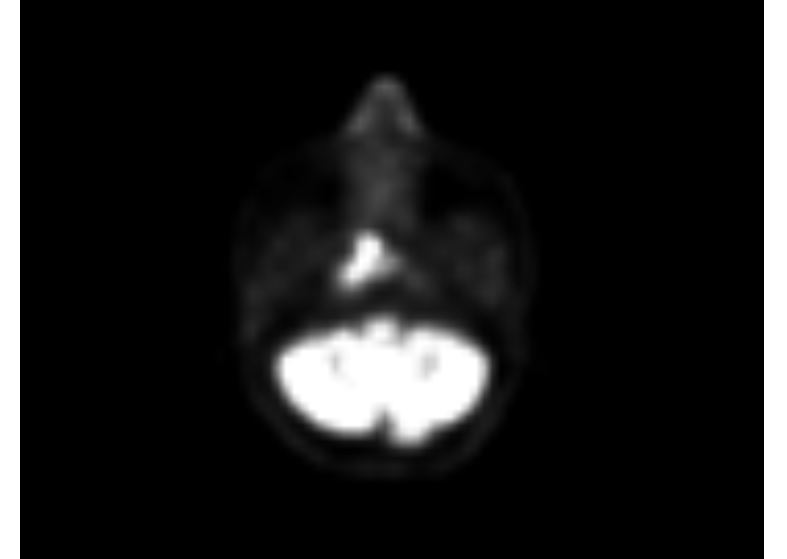
PET- Scan of a patient showing A hyper-metabolic soft tissue lesion measuring 13 x 10 mm is seen in right nasopharynx
Contributed by Abdul Basit
(Click Image to Enlarge)

A CT image of a patient with a Left sided nasopharyngeal mass involving the posterior pharyngeal wall and showing minor opacification of the maxillary antrum bilateral
Contributed by Abdul Basit.
(Click Image to Enlarge)

Staging Table 01
Contributed by Abdul Basit Shah, MBBS
(Click Image to Enlarge)

Staging Table 02
Contributed by Abdul Basit Shah, MBBS
Contributed by Meltem Özdemir, MD