Open Fracture Management
- Article Author:
- Jessica Sop
- Article Editor:
- Aaron Sop
- Updated:
- 8/14/2020 9:10:27 PM
- For CME on this topic:
- Open Fracture Management CME
- PubMed Link:
- Open Fracture Management
Introduction
An open fracture is an injury where the fractured bone and/or fracture hematoma are exposed to the external environment via a traumatic violation of the soft tissue and skin. The skin wound may lie at a site distant to the fracture and not directly over it. Therefore, any fracture that has a concomitant wound should be considered open until proven otherwise.[1][2]
Etiology
Open fractures occur secondary to trauma. They most commonly occur as high-energy injuries, but can also be a result of low-velocity trauma when the sharp ends of the fracture fragments pierce through the skin and soft tissue. High-energy, open fractures are often associated with other life-threatening conditions secondary to poly-trauma and pose other risks such as neurovascular injuries, soft tissue crushing, wound contamination and skin degloving which makes them more likely to have complications.[3]
Epidemiology
A 15-year review of epidemiologic factors of open fractures in adults, reports the incidence was 30.7 per 100,000 persons per year. Motor vehicle accidents are the most common cause of open, lower extremity fractures and are responsible for 34.1% of these injuries. Crush injuries are the most prevalently associated with open, lower extremity fractures causing 39.5% of these cases. The overwhelming majority of open fractures occur singularly, but patients may have more than one at a time. The overall average age of occurrence is 45.5 years, but in general, the incidence declines in males and increases in females with age. The highest incidence of open fractures in males is between ages 15 and 19 years at 54.5 per 100,000 persons per year, whereas the highest occurrence in females is at 53.0 per 100,000 persons per year between the ages of 80 and 89 years. Open phalanx fractures are the most common open fractures accounting for more than 45% of all open injuries. The most common long bone fracture is the tibia and fibula at 11.2%.[4][5][6]
Pathophysiology
When a traumatic injury occurs, bones and soft tissue absorb the imposed energy. It is when the threshold of absorption is exceeded that communication of the bone occurs causing periosteal stripping and soft tissue destruction. The comminuted bone fragments are often not attached to any anchoring structures which allow them to be displaced causing significant soft tissue and neurovascular structure damage. When the skin tears, it creates a vacuum effect which then pulls all surrounding debris into the wound. The foreign material and dirt can often be deposited into deep intramuscular and bone cortex.
History and Physical
Patients with open fractures have a reported history of trauma that is most commonly high velocity in nature. The patient should be adequately undressed to evaluate for other significant, life-threatening injuries per advanced trauma life support protocol. The initial focus should be on assessing the status of the patient's airway, breathing, and circulation, and resuscitation measures should be implemented as necessary. Once the patient has been stabilized, open fractures should be addressed emergently. These injuries are associated with symptoms of pain, deformity, swelling, and a wound that may be bleeding. It should be noted that the wound may not lie directly over the fracture site. The movement and neurovascular status of all involved limbs should be assessed to ascertain whether or not there is a possible nerve or vascular injury associated with the fracture.
The wound should be examined thoroughly and characterized according to the Gustilo-Anderson classification system for open fractures as this will dictate initial treatment. Gustilo-Anderson type I open fractures is a low energy injury with wounds less than 1 cm with minimal soft tissue damage. Type II fractures are low to moderate energy injuries with wounds that are greater than 1 cm with moderate soft tissue and muscle damage. Type III fractures are high-velocity injuries have wounds greater than 10 cm. Type IIIa injuries have severe crushing soft tissue damage, type IIIb have a significant loss of tissue coverage, and type IIIc have significant loss of tissue with an associated vascular injury.
Evaluation
Because patients with open fractures usually sustain significant trauma, an arterial blood gas (ABG), hemoglobin, hematocrit, platelet count, metabolic panel, serum lactate, and toxicology screens are often warranted. Plain radiographs are usually adequate to assess the extent of the fracture. At a minimum, anteroposterior and lateral views of the injured bone should be obtained. The joints above and below the injury should also be x-rayed as the fracture could extend into the adjacent joints or involve articular surfaces. Air present on plain radiographs in the muscle, subcutaneous tissue or joint and visualized foreign bodies indicate an open injury. If the patient is stable, a CT of the ankle or knee joint may be helpful to characterize the orientation of the fracture and aid in reduction and plans for fixation. In the absence of pulses, a CT angiogram can be used to identify vascular injury.[7][8]
Treatment / Management
With significant trauma, resuscitation and stabilization efforts are paramount. After the patient is stabilized, open fractures should be addressed emergently. If there is vascular compromise thought to be secondary to fracture fragments compressing a vessel, reduction of the fracture should be attempted immediately. The wound should be thoroughly irrigated with at least one liter of saline or a combination of saline and betadine, and then a sterile or betadine soaked dressing should be placed over the wound, and the limb should be immobilized in a well-padded splint. Repetitive uncovering of the wound increases infection rates. Antibiotics should be administered as soon as possible in the prehospital setting or emergency department. One study suggested that antibiotic administration within three hours of injury decreases infection rates six-fold. A more recent retrospective study by Lack, et al. indicated that if antibiotics were given within 66 minutes of injury, the infection rate was 0%, but increased to 17% if antibiotics were delayed beyond this time frame. For grade 1 and grade 2 open fractures antibiotics should be given to cover gram-positive organisms. Cephalosporins such as cefazolin or cefuroxime can be used. Additional coverage for gram-negative organisms should be administered in grade 3 fractures. Aminoglycosides such as gentamicin are commonly used in this instance. In the presence of fecal or possible clostridial contamination or if the injury occurred in a farmyard, high dose penicillin should also be given. If a patient is truly penicillin allergic, clindamycin is an acceptable substitute. The tetanus status of all patients with open fractures should be assessed. If a patient has not completed the tetanus series or has not had a booster in the last five years, tetanus toxoid should be given. If the wound is high risk for Clostridium contamination or the patient has not had a tetanus booster in more than ten years, both tetanus toxoid and tetanus immune globulin should be administered.
An orthopedic surgeon should be consulted immediately to start planning for definitive management.[9][10][11]
Complications
- Infection
- Failure to heal
- Non-union
Pearls and Other Issues
Patients with open fractures require definitive operative intervention after emergency stabilization and treatment. In the case that there are other concomitant traumatic injuries, the patients will need to be admitted to a trauma center by a trauma service equipped to manage their condition. Depending on the institutional practice and mechanism of injury, patients with isolated open fractures may be admitted by orthopedic services.
Enhancing Healthcare Team Outcomes
Patients with open fractures usually present to the emergency department; however, unlike the routine closed fracture, these fractures are always serious and need prompt treatment. The triage nurse in the ED must be fully aware of the seriousness of this injury and ensure prompt admission and referral to an orthopedic surgeon. Procedures are well established in most emergency departments on how to manage open fractures. The key is to minimize bacterial contamination of the wound and prompt management in the operating room. The outcomes of open wound do vary depending on the extent of the injury, degree of contamination, time to treatment and patient comorbidity. The latest data indicate that internal fixation does lead to better outcomes in most tibial fractures but in severe injuries, external fixation continues to be the appropriate choice. With prompt treatment, the risk of infection and non-union have also decreased. However, for most patients open fractures are always associated with a prolonged recovery period and most patients do develop some degree of functional disability. [12][13]
(Click Image to Enlarge)
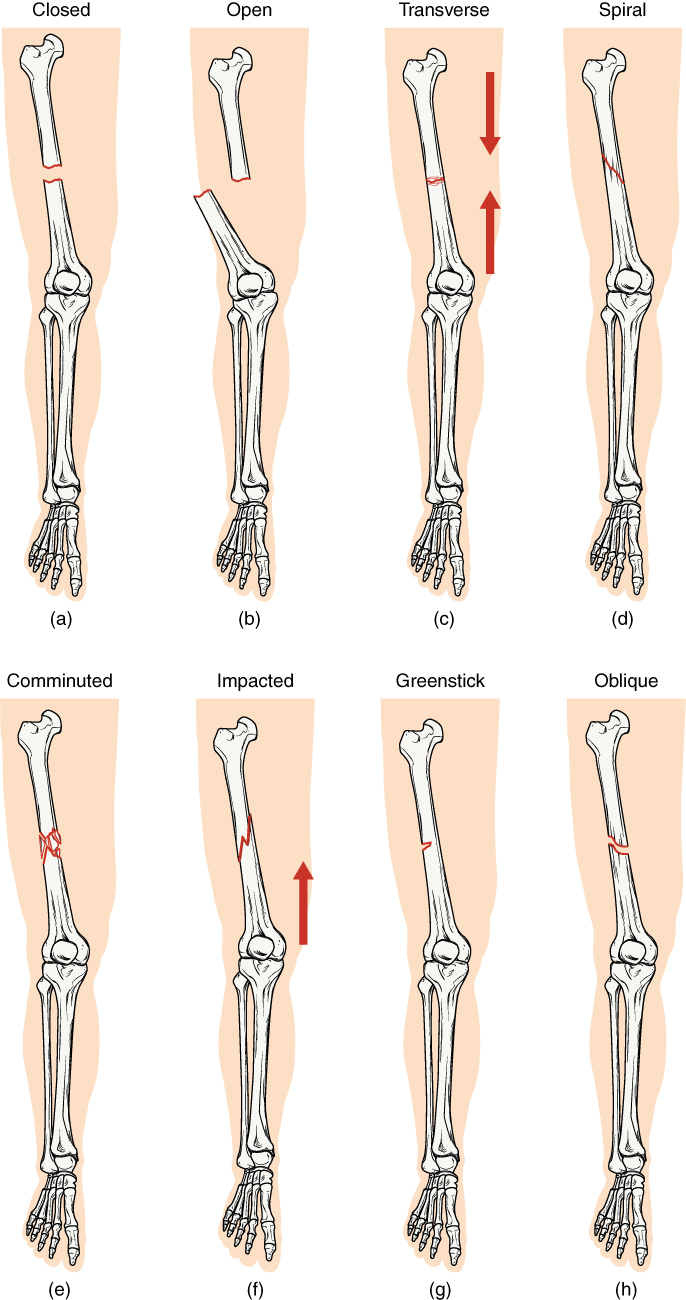
Bone, Different types of fractures, Closed Fracture, Open Fracture, Transverse Fracture, Spiral Fracture, Comminuted Fracture, Impacted Fracture, Greenstick Fracture, Oblique Fracture
Contributed by Wikimedia Commons, OpenStax College (CC by 4.0) https://creativecommons.org/licenses/by/4.0/deed.en
(Click Image to Enlarge)

X-ray, Open Fracture, Broken Arm
Contributed by S.J.Brown, Wikimedia Commons (Public Domain)
(Click Image to Enlarge)

Open Fracture Management Open fracture of the ankle with exposed fibular present. Gustilo Type 2
Contributed by Mark A. Dreyer, DPM, FACFAS
(Click Image to Enlarge)

Open Fracture Management Open fracture of the ankle with exposed tibia present. Gustilo Type 3.
Contributed by Mark A. Dreyer, DPM, FACFAS