Parapneumonic Pleural Effusions And Empyema Thoracis
- Article Author:
- Eman Shebl
- Article Editor:
- Manju Paul
- Updated:
- 8/10/2020 4:47:06 PM
- For CME on this topic:
- Parapneumonic Pleural Effusions And Empyema Thoracis CME
- PubMed Link:
- Parapneumonic Pleural Effusions And Empyema Thoracis
Introduction
A parapneumonic effusion refers to the accumulation of exudative pleural fluid associated with an ipsilateral lung infection, mainly pneumonia. Parapneumonic effusions are mainly associated with bacterial infections.[1]
Parapneumonic pleural effusions are classified into:
- Uncomplicated parapneumonic effusions, which are exudative, neutrophilic effusion. Gram stain and culture are negative, glucose level greater than 60 mg/dl, pH above 7.20.
- Complicated parapneumonic effusions, resulting from a bacterial introduction into the pleura. In this type of parapneumonic effusion, there is a decreased glucose level, pleural fluid is below 7.20. Cultures of fluid from complicated parapneumonic effusions are negative and rapid bacterial clearance from the pleural space, or low bacterial count may explain this. The fluid termed as complicated because it necessitates drainage for resolution.
- Empyema thoracis in which there is frank pus in the pleural space, or there is evidence of bacterial infection of the pleural fluid by Gram stain or a positive culture.[2][3]
Pleural effusions are common in patients who develop pneumonia. At least 40-60% of patients with bacterial pneumonia will develop a pleural effusion of varying severity. Today, these parapneumonic effusions are not common because of prompt antibiotic therapy. However, in some patients the parapneumonic effusion becomes fibrinous and later develops an infection, resulting in an empyema.
Etiology
Pneumonia is the most frequent cause of parapneumonic effusions and empyema thoracis. Empyema may result as a complication of cardiothoracic surgery. Trauma can also lead to infection of the pleural space. The infecting organism may have spread from blood or other organs into the pleural space.[4][5]
Both viruses and bacteria can cause parapneumonic effusions, but it is the latter that is the most common cause of empyema thoracis.
Risk Factors
There are risk factors for empyema like age and comorbidities such as diabetes, alcoholism, GERD, advanced age and repeated hospitalization for pneumonia.[4]
Bacteriology
Streptococcus pneumoniae and Staphylococcus aureus are responsible for about 70% of aerobic gram-positive cultures. Klebsiella, Pseudomonas, and Haemophilus species are the commonest in gram-negative culture. Bacteroides and Peptostreptococcus species are the commonest anaerobic organisms. In empyema thoracis associated with aspiration pneumonia mixed bacterial florae containing aerobic and anaerobic bacteria are common. The common organism in cases of empyema thoracis complicating surgery is S. aureus.[4][6]
A very common cause of infection of the chest cavity is trauma. Any hemothorax that is not adequately evacuated can result in an empyema. Other causes include mediastinitis, ruptured esophagus, pericarditis, pancreatitis, and subdiaphragmatic abscesses.
Epidemiology
Pathophysiology
The stages of parapneumonic effusion are:
- Exudative stage, in which there is an accumulation of fluid in the pleural space due to increased capillary permeability that results from proinflammatory cytokines, such as interleukin 8 (IL-8) and tumor necrosis factor-alpha (TNF-a). The pleural fluid in this early stage is usually clear exudative fluid with a predominance of neutrophils. Pleural fluid in this stage is simple parapneumonic effusion that usually resolves with adequate antibiotic treatment of pneumonia without the need for drainage. This stage takes approximately 2 to 5 days from the onset of pneumonia.
- Fibrinopurulent stage, which can develop if adequate treatment is not provided. In this stage there is a deposition of fibrin clots and fibrin membranes in the pleural cavity, leading to fluid loculations. This stage takes about 5 to 10 days after pneumonia onset.
- Organizing stage, in which fibrin membranes are transformed by fibroblast into a thick nonelastic pleural peel, resulting in the trapped lung with restrictive respiratory dysfunction. This stage may take about 2 to 3 weeks to develop.
The clinical course varies from spontaneous healing to chronic empyema and fibro-thorax with trapped restricted lung.[8]
History and Physical
The clinical manifestations of parapneumonic effusion or empyema are related to various factors like the presentation timing and the virulence of the causative organism. Common symptoms of bacterial pneumonia with parapneumonic effusion include a cough, expectoration, and a rise in body temperature, pleuritic chest pain, and difficulty breathing.
In most patients the following clinical signs are present in clinical examination and include:
- Fever, tachypnea, and tachycardia
- Pleural effusion (dullness to percussion decreased tactile fremitus and decreased or absent breath sounds)
- Adjacent pneumonia (rales or crackles and/or bronchial breath sounds)[9]
Evaluation
Radiographic Investigations
Plain chest x-ray: Pleural effusion can easily be detected by conventional radiographic. The consistency of these pleural-based densities suggests pleural fluid loculation.[1]
Chest ultrasound: Ultrasonography helps identify free or loculated pleural effusions and helps with thoracentesis guidance.[10]
Chest computed tomography (CT): For empyema or loculated effusion in adults, a CT scan with intravenous contrast is helpful. Radiographic contrast enhances the visualization of the pleural surfaces and helps identify pleural fluid loculations. Empyema is suggested by the presence of a split pleura sign in which there is a thickening of the visceral and parietal pleura with significant separation of the pleural surfaces. CT helps in detecting underlying parenchymal abnormalities.[11]
Thoracentesis
A diagnostic thoracentesis is needed for the management guidance of parapneumonic pleural effusion. In general, a parapneumonic effusion should be sampled if It is a free-flowing and layers greater than 10-mm on a lateral decubitus film. Radiological guidance of thoracentesis by ultrasound or chest computed tomography (CT) in some cases is helpful especially when the effusion is loculated.[12] The aspirated pleural fluid is subjected to:
- Microbiologic analysis: Gram stain with cultures and sensitivity (aerobic and anaerobic)
- Pleural fluid total and differential cell count
- Biochemical analysis: Total protein, lactate dehydrogenase, glucose) and pH
- Pleural fluid biomarkers: Novel biomarkers of infection (e.g., C-reactive protein, procalcitonin, STREM-1) have been evaluated to help distinguish complicated parapneumonic pleural effusions from uncomplicated parapneumonic pleural effusions, but there is no proven superiority to traditional pleural biochemistries.[13][14]
More appropriate investigations should be performed to exclude other causes of pleural effusion when indicated.
Treatment / Management
Treatment of parapneumonic effusion includes appropriate antibiotic therapy together with drainage of pleural fluid as indicated.
Parapneumonic effusion is classified into 4 groups based on risk for the poor outcome:
- Category 1 (very low risk): The effusion is small (less than 10-mm thickness on decubitus) and free-flowing. No thoracentesis is indicated.
- Category 2 (low risk): The effusion is small to moderate (equal to 10 mm and less than half the hemithorax) and free-flowing with negative culture and Gram stain regardless of the prior use of antibiotics and pH equal to 7.20.
- Category 3 (moderate risk), in which one of the following criteria is present: the fluid equal to half the hemithorax, loculated effusion, thicken pleura on contrast-enhanced CT scan, positive Gram stain or culture or pH less than 7.20.
- Category 4 (high risk): This is when pleural fluid is in the form of pure pus.
Patients with category 1 and category 2 may not require drainage. In patients with category 3 and 4, drainage is recommended. Fibrinolytics, VATS, and surgery may be indicated for managing patients with category 3 and category 4 parapneumonic effusion not responding to less invasive drainage methods.[12]
Antibiotic Therapy
It must cover the suggested causative organisms of pneumonia according to the clinical setting. The duration of antibiotic therapy depends on many factors, for example, the sensitivity of the organism, extent of pulmonary parenchymal and pleural disease, response to initial therapy and adequacy of drainage.[15]
Chest Tube Drainage
Chest tube drainage is generally preferred for patients with uninoculated effusions and free-flowing fluid. Chest tubes are ideally inserted under ultrasound or CT-guidance. The choice of a thoracostomy tube size is controversial. Imaging performed within 24 hours is essential for documenting the correct position of the chest tube. Chest tubes are left in place until the drainage rate is less than 50 ml per day and the empyema cavity has closed.[15]
Fibrinolytic Agents
The intrapleural administration for fibrinolytic agents (for example, streptokinase and tissue plasminogen activator) or fibrinolytic plus mucolytic agents aiming for facilitating the drainage of the loculated parapneumonic effusion is controversial.[16][17]
Thoracoscopy
Thoracoscopy is an alternative therapy for loculated empyemas when antibiotics and tube thoracostomy fail for the drainage. Thoracoscopy disrupts the intrapleural adhesions and allows the drainage of the pleural fluid.[18] Previous studies showed that delay for referral for thoracoscopy more than two weeks was associated with failure of thoracoscopy and conversion to thoracotomy.[19]
Decortication
Decortication is indicated when persistent (present after 6 months) pleural peel is formed, leading to significant pulmonary restriction.[20]
Rib Resection and Open Drainage of Pleural Space
A vertical incision through the chest wall with rib resection (1 to 3) is done to allow pleural fluid drainage. A chest tube is left in place (about 60 to 90 days). Open drainage of the pleural space may be considered when the previous methods fail, and when the patient is too ill to tolerate decortications.[20]
Differential Diagnosis
- Bacterial pneumonia
- Perforated esophagus
- Hemothorax
- Chylothorax
- Lung cancer
- Tuberculosis
Prognosis
Most of the patients with parapneumonic pleural effusion recover, but the mortality rate still around 10%. Proper antibiotic therapy and pleural fluid drainage are vital for recovery.[1] Scoring systems have been studied (RAPID score) to determine which patients with parapneumonic effusions are at the highest risk for a poor outcome.[21]
Other factors that complicate treatment include patient age, cardiac and respiratory compromise, immunosuppression, and frailty. Overall, death rates are higher in older patients.
Complications
Complications of pleural empyema may include residual pleural thickening, extensive pleural fibrosis, bronchopleural fistula formation, and development of empyema necessitans.[22]
The surgery is also associated with numerous complications including pain, recurrence, prolonged hospital stay, injury to the chest organs, diaphragmatic paralysis and fractured ribs.
Pearls and Other Issues
Early diagnosis, appropriate antimicrobial therapy, and adequate drainage of parapneumonic effusion are essential for decreasing its morbidity and mortality.
Enhancing Healthcare Team Outcomes
The parapneumonic pleural effusion management requires interprofessional cooperation between physicians of the concerned specialties (e.g., pulmonary medicine, radiology, and microbiology and cardiothoracic surgery) for a good outcome. The interprofessional care provided to the patient must follow an evidence-based approach. [Level 3]
(Click Image to Enlarge)

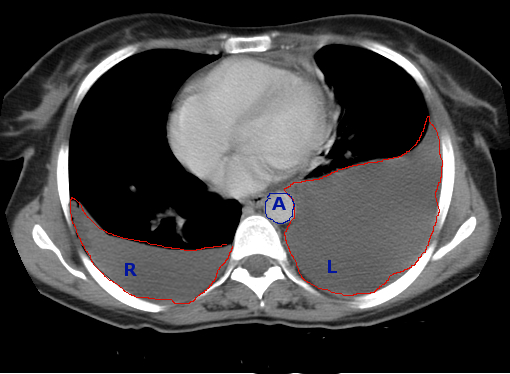
CT Chest bliateral Plueral Effusions
Contributed by Scott Dulebohn, MD
(Click Image to Enlarge)
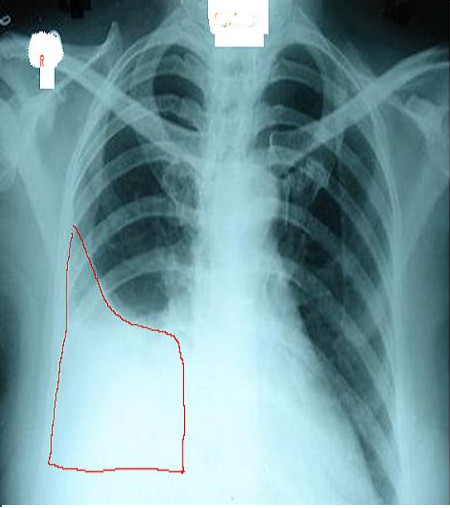
Right Pleural Effusion, X-ray
Contributed by Steve Bhimji, MS, MD, PhD
(Click Image to Enlarge)
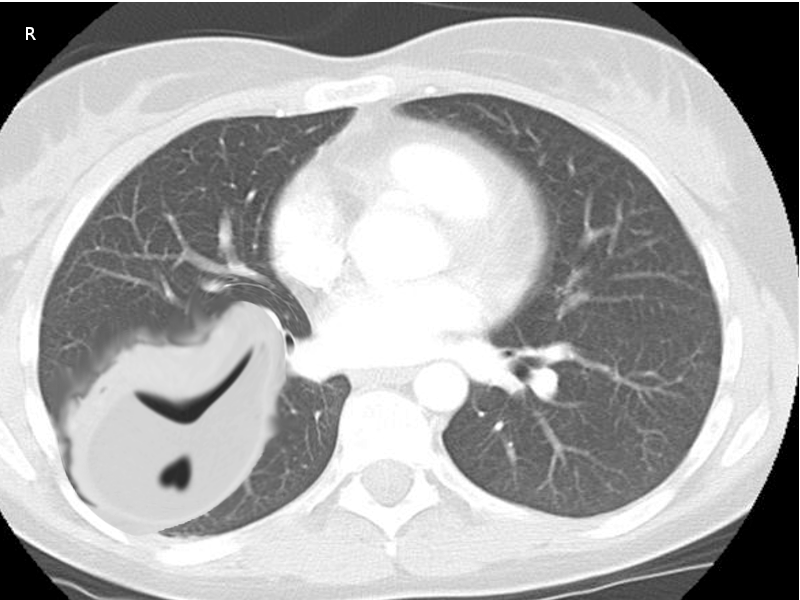
CT scan of chest effusions
Image courtesy S Bhimji MD
(Click Image to Enlarge)
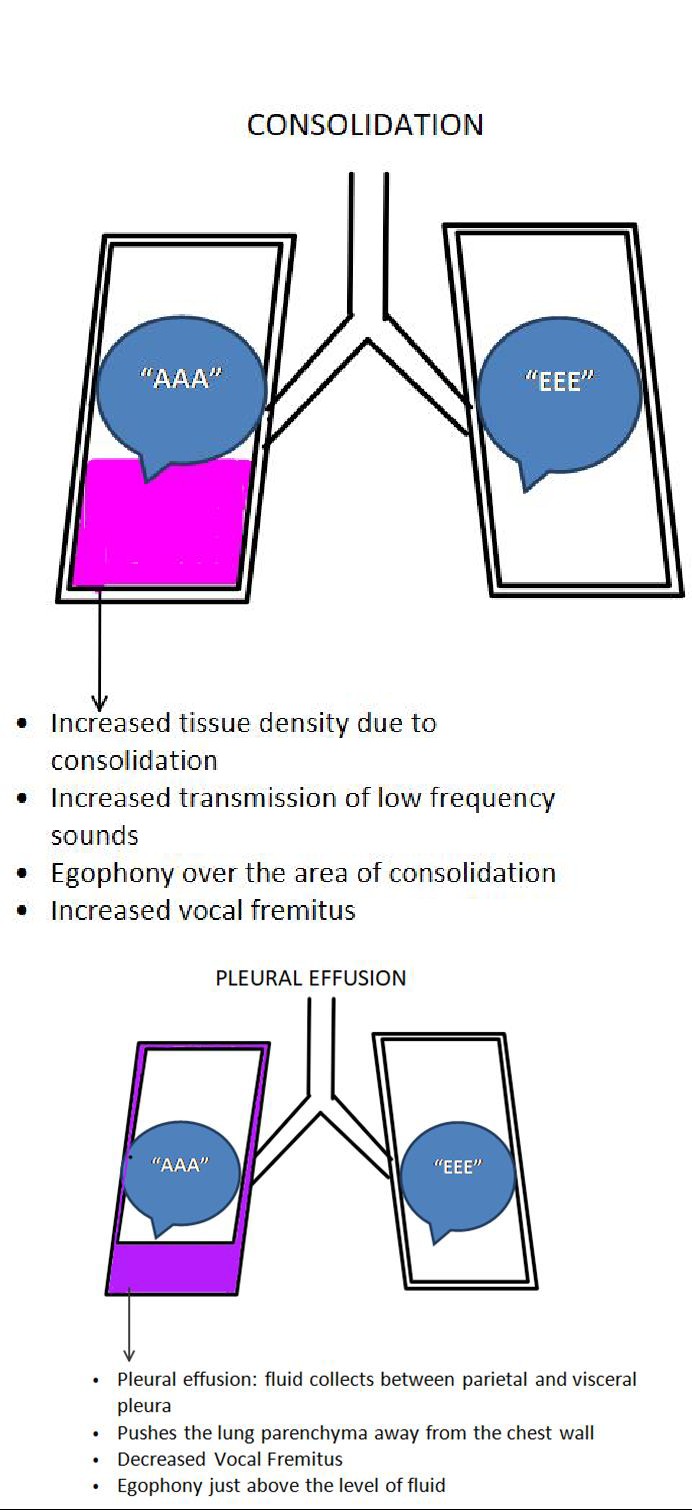
Consolidation and Plueral Effusion
Contributed by Pranav Modi
(Click Image to Enlarge)
Empyema chronic
Image courtesy Dr Chaigasame