Anatomy, Bony Pelvis and Lower Limb, Piriformis Muscle
- Article Author:
- Carol Chang
- Article Author:
- Susan Jeno
- Article Editor:
- Matthew Varacallo
- Updated:
- 10/28/2020 1:08:13 AM
- For CME on this topic:
- Anatomy, Bony Pelvis and Lower Limb, Piriformis Muscle CME
- PubMed Link:
- Anatomy, Bony Pelvis and Lower Limb, Piriformis Muscle
Introduction
The piriformis is a flat, pear-shaped muscle located in the gluteal region of the hip/proximal thigh. It is one of the six short external rotator group muscles in the glulteal region of the proximal thigh. It courses parallel to the posterior margin of the gluteus medius, deep to gluteus maximus. The piriformis muscle has origins from several anatomical locations including the anterior surface of the lateral process of the sacrum, the spinal region of the gluteal muscles, and the superior/gluteal surface of the ilium near the margin of the greater sciatic notch, the capsule of the adjacent sacroiliac joint and sometimes from the sacrotuberous ligament. The muscle passes from the pelvis to the gluteal region by passing through the greater sciatic notch and inserts on the medial side of the superior aspect of the greater trochanter of the femur. The tendon of the piriformis muscle joins the tendons of the obturator internus and the inferior and superior gemellus (i.e. the conjoint tendon) before inserting on the femur. The muscle abuts the posterior wall of the pelvis and the posterior wall of the hip joint.[1][2]
Piriformis syndrome is a neurological disorder that often presents with hip and buttock pain.[3]The syndrome is often misdiagnosed and undertreated.
Structure and Function
The piriformis muscle is an external (or lateral) rotator of the hip along with the superior and inferior gemellus, quadratus femoris, and obturator internus and externus. The piriformis muscle rotates the femur during extension of the hip and abducts the femur during flexion of the hip. The abduction of the femur is critical during walking as it shifts the body weight to the opposite side, which prevents one from falling.[4][5]The piriformis muscle also serves as a landmark in the gluteal region. As it passes through and nearly completely fills the greater sciatic foramen, the muscle divides the foramen into a superior and inferior segment. This anatomy also helps name the nerves and vessels of the region. The superior gluteal nerve and artery exit superior to the piriformis. The inferior gluteal nerve and artery exit inferiorly. All other nerves and vessels exit the pelvis inferior to the piriformis. The sciatic nerve generally exits the pelvis inferior to the piriformis muscle, however, variations do occur and the entire never may pass superior to or through the muscle. In other variations, the sciatic nerve may be split into its major divisions which may lie on either side of the piriformis, or one division can pass through the muscle with the other division above or below the muscle belly.
Embryology
The limb buds appear at four weeks as tiny masses on the ventrolateral body wall. Reciprocal induction of ectoderm and mesoderm forms the limb buds. Each bud is initially composed of a mass of mesenchymal cells covered by ectoderm. As the limb bud grows, it receives innervation from the last four and first three sacral metameres. As the distal limb end flattens into foot plates, grooves appear in the limb. Rotation of the foot plate occurs so that it aligns with the fibula and tibia by week 9 to 12. At the same time, the muscles start to grow on the flexor and extensor surfaces of the limb.
Blood Supply and Lymphatics
The limb buds appear at four weeks as tiny masses on the ventrolateral body wall. Reciprocal induction of ectoderm and mesoderm forms the limb buds. Each bud is initially composed of a mass of mesenchymal cells covered by ectoderm. As the limb bud grows, it receives innervation from the last four and first three sacral metameres. As the distal limb end flattens into foot plates, grooves appear in the limb. Rotation of the foot plate occurs so that it aligns with the fibula and tibia by week 9 to 12. At the same time, the muscles start to grow on the flexor and extensor surfaces of the limb.
Nerves
Piriformis is innervated by branches of the anterior rami of S1 and S2 of the sacral plexus. In some instances, the muscle will be supplied by only S2 and in other cases there may be contributions from L5 nerve roots. In at least a fifth of the population, the piriformis is pierced in different parts by the sciatic nerve. However, in some cases, it may be penetrated by the common fibular nerve. In a few people, the muscle may integrate with the gluteus medius and minimus muscles. The piriformis may also have one or two attachments to the sacrum or capsule of the hip joint.[6][7]
Muscles
The piriformis muscle is intimately associated with gluteus medius, gluteus maximus, obturator internus, and the gemelli muscles.
Physiologic Variants
In about 20% of the population, the sciatic nerve or its branches innervate the piriformis muscle. There are many nerve variations, but in about 80% of people, the common fibular nerve penetrates the muscle.
Sometimes the anatomy of the piriformis muscle may not be clearly defined. This lack of definition occurs because the muscle may have merged with the gluteus medius or gluteus minimus.
Surgical Considerations
Surgical release is only given consideration in refractory conditions after nonoperative modalities are exhausted.
The open surgical approach entails the complete release of the piriformis tendon from its insertion on the posterior femur. In addition, neurolysis of the sciatic nerve is often performed in tandem. The latter is recommended in the setting of advanced/severe fibrotic conditions adversely affecting the course of the nerve itself.
In general, the outcome after surgery depends on the chronicity of the condition, but results are often variable. Patients should be counseled prior to the surgery regarding the risk of continued pain/symptoms even after the surgical procedure is performed.
All patients with piriformis syndrome should enroll in a physical therapy program. The patient should undergo stretching and motion exercises to help relieve the adhesions on the nerve. The goal should be to eliminate symptoms and improve function.
Clinical Significance
Piriformis syndrome is a nondiscogenic cause of compression neuropathy affecting the sciatic nerve at the level of the ischial tuberosity. [8][9][10]
The condition is often misdiagnosed and undertreated. Buttock pain is often confused with sciatica, sacroiliitis, lumbar radiculopathy, or trochanteric bursitis. The number of patients with piriformis syndrome has dramatically increased over time. The condition accounts for many cases of partial or total disability. When there is a delay in diagnosis, it leads to chronic pain, hyperesthesia, paresthesias, and muscle weakness.
Piriformis syndrome is associated with pain in the buttocks with sporadic, referred pain along the distribution of the sciatic nerve. Individuals in whom the sciatic nerve pierces the piriformis muscle are prone to sciatica. Sciatica will present with tingling, numbness, or pain deep in the buttock area and along the sciatic nerve. Prolonged sitting, climbing stairs, stretching, and performing squatting can also worsen the pain. The patient's history and clinical exam make the diagnosis of piriformis syndrome. MRI and nerve conduction studies are done to exclude other pathologies. Once diagnosed, piriformis syndrome is treated with physical therapy and stretching exercises. Rarely, corticosteroids or botulinum toxin may be injected into the piriformis muscle. Surgery for nerve decompression is the last resort for the treatment of piriformis syndrome.
Other Issues
Pharmacological therapy is often the first therapy in patients with piriformis syndrome. Both NSAIDs and prescription analgesics are used to treat the condition with varying results. Overall, some studies indicate that NSAIDs are preferred to opiates and tend to work well.
Muscle relaxants have also been used to manage patients with piriformis syndrome. While these agents do work, they are also associated with many serious adverse effects like drowsiness, dry mouth, and dizziness.
Osteopathic manipulation is often recommended for patients with piriformis syndrome. Both direct and indirect osteopathic manipulative treatments are used to facilitate a normal range of motion and relieve pain.
Steroid injections have also been used to treat piriformis syndrome. The steroids are thought to act by decreasing the inflammation around the nerve. However, evidence to support the use of steroid injections in chronic cases is lacking. A common complication of steroid injections in many studies has been an infection.
(Click Image to Enlarge)

Piriformis, Sciatic Nerve, Obturator Internus
Contributed Illustration by Beckie Palmer
(Click Image to Enlarge)
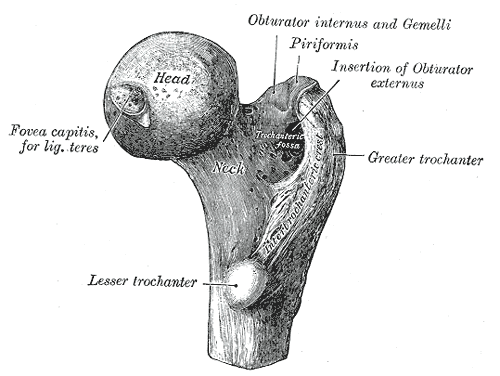
Femur, Right, Upper Extremity, Head, Fovea capitis, Ligament teres, Neck, Obturator internus, Gemelli, Piriformis, Obturator externus, Trochanteric Fossa, Trochanter, Lesser Trochanter, Greater Trochanter, Intertrochanteric Crest.
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)
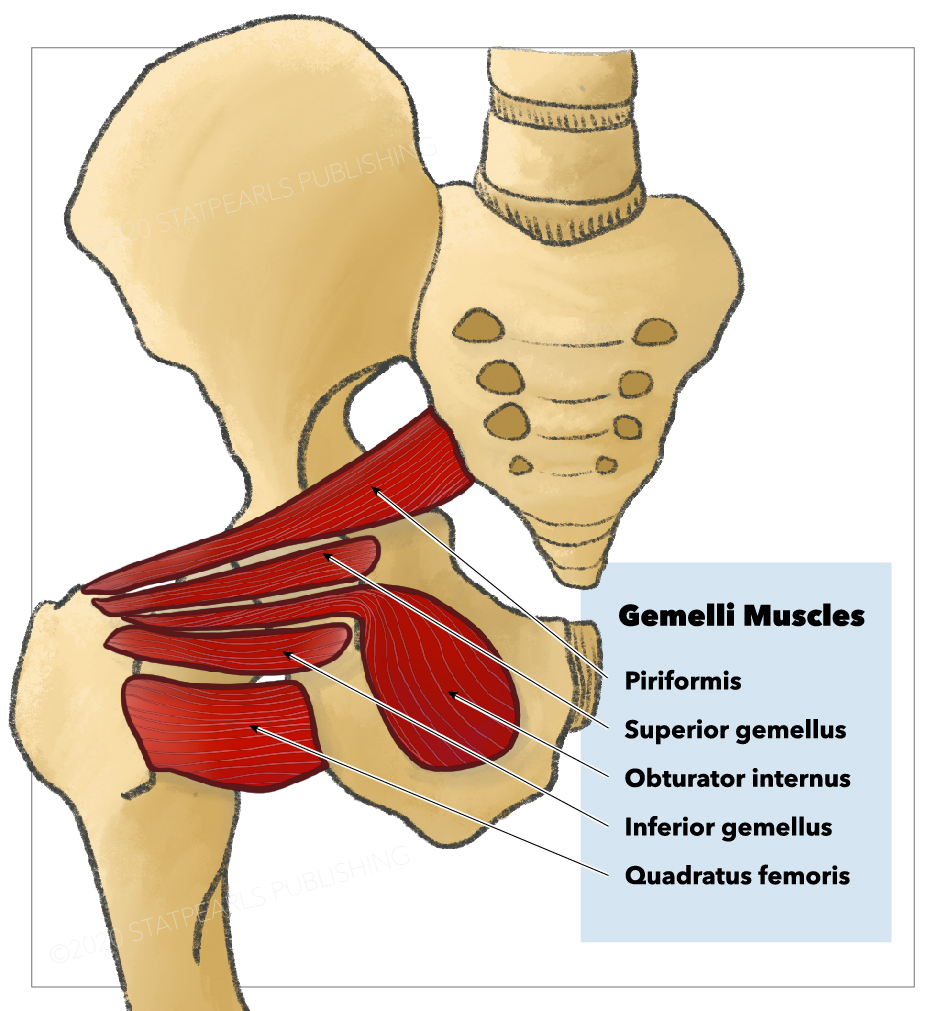
Gemelli muscles, Quadratus femoris, Obturator internus, Inferior gemellus, Superior gemellus, Piriformis
StatPearls Publishing Illustration