Posterior Cerebral Artery Stroke
- Article Author:
- Okkes Kuybu
- Article Author:
- Prasanna Tadi
- Article Editor:
- Rimal Dossani
- Updated:
- 8/10/2020 8:52:18 PM
- For CME on this topic:
- Posterior Cerebral Artery Stroke CME
- PubMed Link:
- Posterior Cerebral Artery Stroke
Introduction
A solid understanding of the pathophysiology of a posterior cerebral artery (PCA) stroke as well as the syndrome relating to it, requires adequate knowledge of the structures and vascular anatomy of the brain. Anterior and posterior circulations provide the primary blood circulation of the brain. Both circulations are connected by the posterior communicating arteries (PCOM), which make up the circle of Willis. When there is an occlusion in the cerebral vasculature, the circle of Willis, as well as collateral circulations, provide blood to the occluded areas. Posterior circulation is supplied by the vertebral arteries (VA), posterior inferior cerebellar arteries (PICA), basilar artery (BA), anterior inferior cerebellar arteries (AICA), pontine branches of the basilar artery, superior cerebellar arteries (SCA), PCA, and PCOM. The VAs arise from the subclavian arteries and fuse into the BA within the cranium. The BA typically divides into PCAs near the pituitary stalk at the pontomesencephalic junction. PCAs can originate from BA 70 percent of the time, 20 percent of the time from PCOMs, and 10 percent of the time from a mix of the two.[1] The PCAs then give off branches to the midbrain, subthalamic nucleus, basal nucleus, thalamus, temporal, occipital, and occipitoparietal cortices (See Figure).
PCA is divided into four segments, P1 to P4. The segments can be further categorized into deep and superficial segments or proximal and distal, respectively.
- P1 and P2 segments are deep segments. The P1 segment is between the termination of the BA and the PCOM. The thalamic-subthalamic arteries derived from the P1 segment supply the paramedian parts of the upper midbrain and thalamus. The tuberothalamic arteries usually arise from the PCOM and supply the anterior and anterolateral parts of the thalamus. Both sides of the thalamus and midbrain can be supplied by an Artery of Percheron (AOP), which is a rare anatomic variation. AOP arises from proximal P1.[2][3] The other branches of the P2 segment include thalamogeniculate arteries and the posterior choroidal arteries. The thalamogeniculate arteries supply the ventrolateral part of the thalamus. The posterior choroidal arteries supply the lateral geniculate body, pulvinar, posterior thalamus, hippocampus, and parahippocampal gyrus.
- P3 and P4 are superficial segments. The P3 segment is the quadrigeminal segment. Anterior and posterior inferior temporal arteries arise from the P3 segment. The P4 segment is the cortical segment within the calcarine fissure and became the calcarine artery. Other branches include the occipitotemporal and occipitoparietal arteries.
Etiology
The mechanism of PCA strokes are variable and include large artery disease, small artery disease, atherothrombosis of PCA, BA and VA, embolism (cardiac, aortic, coagulopathy), dissection, hemorrhagic, migraine, Moyamoya disease, fibromuscular dysplasia (FMD), mitochondrial disease, reversible cerebral vasoconstriction syndrome, vertebrobasilar dolichoectasia (VBD), and vasculitis as well as central nervous system (CNS) infections. The most common causes are still atherosclerosis, embolism, and small artery disease.
- Thromboses, that are generated from atherosclerotic arteries (VA, BA, and proximal PCA), is the main pathology of large artery disease. A study of 79 patients with infarcts in one or more cortical territories of the PCA shows 25 (32%) patients with proximal arterial disease. VA atherosclerosis is the most common cause with 18 patients including extracranial and intracranial, followed by 4 patients in the BA.[4]
- Studies are lacking that show small artery disease as a cause of PCA infarcts. Lacunar infarction was the most frequent stroke subtype 80/232 (34.5%) in the Sagrat Cor Hospital of Barcelona Stroke Registry during 19 years between 1986 and 2004.[5]
- A cardiac embolism is the most common etiology of embolism. It includes valvular disease, atrial fibrillation (the most common etiology of cardiac embolism), left atrial or ventricular thrombus, dilated cardiomyopathy, patent foramen ovale (PFO), and congestive heart failure. A cardiac embolism is a reason for pure PCA infarcts in 58/122 (48%).[6]
- A VA dissection is reported to occur more often than PCA dissection.[7]
- The diagnosis of a migrainous stroke is challenging. Studies show that PCA strokes may be due to a migraine, but patients typically have thrombotic arterial occlusions or PFO. A study of 117 patients with strokes in the superficial territory of the PCA included 4 patients (3.4%) with a history of migraines.[8]
- Intracranial involvement in the setting of FMD is a rare condition. FMD of the basilar artery presented with multiple cerebral infarctions which included the PCA territory.[9]
- Patients with the syndrome of mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes (MELAS) typically have mutations at the base pair 3243 (A3243G) of their mitochondrial DNA (mtDNA). Four young patients were diagnosed with clinical and molecular evidence of mitochondrial disease (mtDNA:3243) in a study with 38 patients with occipital stroke (18 to 45 years old).[10]
- Dolichoectasia means elongation and distension. Vertebrobasilar Dolichoectasia (VBD) is another occasional cause of PCA stroke.[11]
Epidemiology
Stroke, a leading cause of adult disability,[12] is the fifth leading cause of death in the United States. Each year, nearly 800,000 people experience a new or recurrent stroke as well as nearly 140,000 deaths each year. There are approximately 7 million stroke survivors. A stroke is reported every 40 seconds, and every 4 minutes someone dies from a stroke. The risk of experiencing a first stroke is nearly twice as high for African Americans as Caucasians, and African Americans also have the highest rate of death due to stroke.[13]
The incidence of PCA strokes can be estimated between 5% to 10%.[1] Some studies include only pure PCA. One study shows that pure PCA strokes account for 232 (6.1%) cases of stroke (n = 3808). Other factors, such as being male and the mean age, are also shown in the same study 128/232 (55.2%) and 73.9 (11.9 SD), respectively.
Pathophysiology
Patients may present with different signs or symptoms when PCA restricts the blood supply of multiple brain regions (the occipital lobe, the inferomedial temporal lobe, a large portion of the thalamus, and the upper brainstem and midbrain). Signs and symptoms may change in a patient with PCA syndrome based upon the location and severity of the occlusion,
- If there is a deep/proximal occlusion, ischemia may be in the thalamus and/or midbrain, as well as in the cortex.
- If there is a well-developed PCOM for collateral flow, proximal occlusion may not produce significant infarction.
- If there is a superficial/distal occlusion of PCA, ischemia may be in only cortical structures.
- If there is well-developed collateral flow in a chronic intracranial atherosclerosis process, the thrombotic occlusion may not produce whole-territory infarction. Cardioembolic may produce significant infarct due to a lack of collateral flow in the acute process.[14]
It is essential to understand the mechanism of stroke. Acute and chronic management, preventive measures can be instituted.
- Atherothrombosis can cause an artery-artery embolism, complete branch, or in situ occlusion and hemodynamic instability.
- Small artery disease includes lipohylinosis and hyaline arteriolosclerosis of small arteries. It is likely due to hypertension, diabetes, and aging.
Symptoms associated with PCA strokes like diplopia, visual field defects, dysphagia, vertigo, alteration in consciousness, memory impairment, or difficulty reading may help us to understand the localization of stroke.[15]
Visual Field Defects
- PCA and deep branches of MCA supply the optic radiations. The lower part of the optic radiations receives blood supply from the PCA. The upper part gets blood supply from the MCA.
- Unilateral infarctions of the occipital lobe may cause contralateral homonymous hemianopia with macular sparing.
- Quadrantanopia may be seen if the defect is limited. If there is an infarction in the temporal lobe involving the Meyer loop or infracalcarine, it may present with superior quadrantanopia. Inferior quadrantanopoia is caused by infarctions in the optic radiation of the inferior parietal lobe or supracalcarine. In a study with pure superficial PCA strokes in 117 patients, 26 (22%) presented with quadrantanopia. Twenty (17%) is superior.[8]
- Visual field defects (hemianopia, quadrantanopia, sectoranopia), hemisensory deficit, and neuropsychological dysfunction (transcortical aphasia, memory disturbances) may be seen after occlusion of the posterior choroidal artery.[16]
- Bilateral infarction of the occipital lobes may cause cortical blindness. The patient may have visual anosognosia.[17] The patient is not aware of her/his deficit. The patient may confabulate and deny blindness.
Visual Dysfunction
- Visual Agnosia: Patients may not understand or describe uses for the objects seen. Patients can name objects when they touch them or when the objects are described to them. The two forms of visual agnosia are apperceptive and associative. Apperceptive involves poor perception and ability to understand while associative involves a poor ability to match and use. It is caused by a large left PCA stroke, which likely causes a disconnect between language and visual systems.[18]
- Prosopagnosia is difficulty recognizing familiar faces due to lesions in the inferior occipital areas, fusiform gyrus, and the anterior temporal cortex.[19] In literature, deficits are shown in the right PCA territory only.[20]
- Alexia refers to difficulty in reading. Alexia without agraphia (pure alexia) is caused by a lesion to the dominant occipital lobe and splenium of the corpus callosum and is often accompanied by right homonymous hemianopia.
- Achromatopsia refers to difficulty perceiving colors. It is due to infarctions in the ventral occipital cortex and/or infracalcarine. The patient may present with hemiachromatopsia if the infarction is unilateral.[21] Tests to check for achromatopsia are Ishihara color plates or the Farnsworth-Munsell 100-hue test.
Cognitive and Behavioral Dysfunction
- Aphasia can be due to an infarction large enough to cover the left parietal lobe or temporal lobe. Transcortical sensory aphasia is caused by infarctions to the parietal-occipital region on the left side. The patient may have amnestic aphasia (inability to name but repetition and comprehension intact) due to infarction to the left temporal lobe of PCA territory.
- Memory impairment is caused by infarction of the hippocampus and parahippocampus.
- Aggressive behavior can be caused by PCA strokes as well. In a study 41 PCA stroke patients, 3 (7.3%) patients showed aggressive behavior such as shouting obscenities and hitting and bitting others.[22] These patients may become anxious, aggressive, and frustrated when they are stimulated by the environment.
- Hallucinations are uncommon but may develop from PCA strokes to any side of the brain.
- Palinopsia refers to seeing images persist even after an image has been removed. Infarctions can be in the lingual and fusiform gyri.
Other Dysfunctions
- Midbrain infarction may present differently, depending on the location of infarction. Patients may present with ataxic hemiparesis due to an anterolateral midbrain infarction or oculomotor or pupillary problems due to a paramedian rostral midbrain infarction.
- Pure sensory stroke may result from a lesion in the ventral posterolateral nucleus, which receives the blood supply from thalamogeniculate (inferolateral) arteries.
- Infractions to the artery of Percheron infarction can result in bilateral paramedian thalamus infarction with or without midbrain involvement. Patients may present with confusion, hypersomnolence, dysarthria, amnesia, and ocular movement disorders.
- Balint syndrome is caused by infarctions to the bilateral occipitoparietal border. This presents with optic ataxia (inability to reach targets one is looking at), oculomotor apraxia (inability to intentionally move eyes towards an object), and simultagnosia (inability to synthesize objects within a visual field).[23][24][23]
- Anton syndrome is due to a sudden onset of bilateral occipital strokes leading to cortical blindness. The patient will deny the blindness.[25]
History and Physical
Stroke is an emergency, and the timing of the onset of symptoms is the most important information in acute settings. Time of onset can be challenging in posterior circulation strokes because patients may be unaware of their symptoms. If a patient is unaware of having symptoms, at practitioner should ascertain when the patient last appeared and behaved in the manner that they were known or accustomed. Once this question is answered, a brief history of presentation and complete physical exam should be obtained. When taking a history, there should be an emphasis on determining the risk factors for stroke in the patient's past medical history. The two main categories of risk factors are non-modifiable and modifiable.
- Non-modifiable risk factors include age, gender (male>female), race (higher in African-American), history of transient ischemic attack (TIA), cerebrovascular disease (CVA), and hypercoagulable states, as well as a family history of hypercoagulable state or CVAs.
- Modifiable risk factors include hypertension, diabetes mellitus, hyperlipidemia, smoking, heart disease (atrial fibrillation, endocarditis) oral contraceptives, substance abuse (cocaine), poor diet, obesity, immobility, and sleep apnea.
Patients may present in a comatose state via ambulance or may walk to an emergency department without assistance. Patients with a PCA stroke may present with only a headache and mild visual changes such as vision loss, diplopia, inability to see half of the view, or difficulty reading perceiving colors, or recognizing familiar faces. Mild symptoms in the setting of a PCA stroke may delay a patient from getting medical treatment. Many times, they are also unaware of their visual problems. Patients may report visual problems such as grayness, spots, voids, and difficulties focusing.[26] Patient history may include unilateral weakness, sensory deficits, language dysfunction, dizziness, nausea, vomiting, cognitive, and behavioral disturbances.
A physical exam is performed as soon as a physician sees the patient. The National Institutes of Health Stroke Scale (NIHSS) is a systematic assessment tool that provides a quantitative measure of stroke-related neurologic deficits. NIHSS gives us a brief evaluation of acuity, determination of appropriate treatment, and can predict patient outcomes. It should be completed in less than 10 minutes and ranges from 0 (no deficit) to 42 (maximum). Posterior circulation strokes, including PCA strokes, may be underestimated by NIHSS when compared to anterior circulation strokes.[27] For example, a patient with complete homonymous hemianopsia has only two NIHSS points, but the patient might have a significant infarct in the occipital cortex, and their daily life will be affected drastically.
A full neurological exam is still essential for a better understanding. A cardiovascular exam also should be performed to check for carotid bruits and abnormal rhythm or heart sounds as well as signs of a DVT. The physical exam may show:
- Homonymous Hemianopia with macular sparing
- Superior or inferior quadrantanopia
- Paresthesia
- Visual complete loss or visual anosognosia
- Visual Agnosia
- Prosopagnosia
- Alexia without agraphia (pure alexia)
- Achromatopsia
- Transcortical sensory aphasia
- Amnestic aphasia
- Memory impairment
- Aggressive behavior
- Hallucinations
- Palinopsia
- Hemiparesis with/without ataxia
- Oculomotor or pupillary deficits
- Hypersomnolence
- Optic ataxia, oculomotor apraxia, and simultagnosia
Evaluation
PCA and other posterior circulation strokes are more difficult to diagnose because of nonspecific and fluctuating symptoms at presentation. Time of onset it essential for further evaluation with tests. In the acute setting, management should begin after obtaining the following:
- Vitals
- Finger-stick blood glucose
- Initial non-contrast head computerized tomography (CT)
The Alberta Stroke Program Early CT Score (ASPECTS) system is a simple and reliable 10-point scale for evaluating early ischemic changes in acute middle cerebral artery stroke. ASPECTS is modified to pc-ASPECTS for the posterior circulation strokes.[28] Points are lost for each area affected such as thalamus (1 point each), occipital lobes (1 point each), midbrain (2 points), pons (2 points), and cerebellar hemispheres (1 each point).
Blood Workup
Tests should include a complete blood count (CBC), prothrombin time (PT), activated partial thromboplastin time (aPTT), international normalized ratio (INR), electrolytes, comprehensive metabolic panel (CMP), troponin, lipid panel, and A1c. Additional tests can be ordered such as ANA with titers, ESR, CRP, ANCA for vasculitis, hypercoagulable panel for coagulopathy, and genetics tests for an unknown cause of stroke after the first workup.
Imaging
In many cases, noninvasive imaging may be enough for diagnosis and management. Stroke imaging includes CT, magnetic resonance imaging (MRI), CT angiogram (CTA), MRA, doppler ultrasound, PET, and SPECT. A four-vessel angiogram can be ordered when unclear findings or more information is needed.
Cardiovascular Test
In most cases, cardiac pathology should be ruled out with the following test: electrocardiogram, chest X-ray, transthoracic echocardiogram, transesophageal echocardiogram, Holter monitoring, and extensive cardiac monitoring.
Treatment / Management
2018 AHA/ASA guidelines address prehospital care, urgent and emergency evaluation, and treatment with intravenous (IV) and intra-arterial therapies for acute ischemic stroke (AIS).[29] Patients with AIS should be checked for airway, breathing, and adequate oxygenation. Intravenous tissue plasminogen activator (tPA) can be administered up to 4.5 hours after AIS. Eligibility recommendations in the 2018 guidelines should be checked before administering IV tPA. The guidelines suggest that the patient must have a blood pressure less than 180/110, finger-stick glucose more than 50 mg/dL, and absence of hemorrhage on initial non-contrast head CT. The dose of tPA is 0.9 mg/kg; the maximum dose is 90 mg over 60 min with an initial 10% of the dose given as a bolus over 1 min.
A patient with AIS may present after a 4.5-hour window and might still be a candidate for endovascular treatment (EVT), which may include angioplasty, stenting, mechanical embolectomy, or intra-arterial thrombolysis. Randomized trials have shown the safety and efficacy of intra-arterial thrombolysis given within 6 hours of symptom onset of AIS. The DAWN and DEFUSE 3 trials selected patients presenting after 6 hours for treatment using imaging-based criteria.[30][31] Unfortunately, the results of this study apply to patient MCA or internal carotid artery (ICA) occlusions. A randomized study on posterior circulation AIS treated with intra-arterial therapy was terminated prematurely because of poor recruitment.[32] The Basilar Artery International Cooperation Study (BASICS) group completed an observational registry study on 619 patients with BA occlusion to see any superiority of intra-arterial therapy to intravenous thrombolysis.[33] The study did have all the limitations of a non-randomized study. Intra-arterial therapy was more accessible every other day. Following this study, a randomized trial for BA occlusion began in 2011 and is still active. The results of the trial may support other possible studies in the future such as a trial of PCA strokes. Despite the lack of information, there are still good outcomes with some case series in literature after intra-arterial therapy for PCA stokes. Intra-arterial thrombolysis is superior to intravenous thrombolysis in 18 patients with isolated PCA.[34] There is a case study with isolated PCA that also underwent an endovascular clot aspiration with significant improvement in the patient's symptoms.[35] Briefly, challenging factors in the acute treatment of PCA stroke include an unclear time of symptom onset, the small size of the vessel, low NIH stroke scale, and the lack of specific guidelines.
The rest of the treatment should be focused on preventing further cerebrovascular accidents. Antiplatelet or anticoagulation should be started based on the etiology of the stroke. Other secondary risk factors should be addressed with better-controlled hypertension, cholesterol, and diabetes.
Differential Diagnosis
- Hypoglycemia
- Hypotension
- Mass in the occipital, temporal, or parietal area
- Migraine
- Multiple sclerosis
- Other types of stroke due to different locations such as vertebrobasilar stroke, lacunar stroke, or MCA stroke.
- Seizure with a postictal state
- Subarachnoid hemorrhage
- Subdural hematoma
- Todd paresis
- Vasculitis
Prognosis
Stroke is a leading cause of disability and the fifth leading cause of death in the United States. The disability and mortality are less likely from pure PCA stroke compared to other strokes.[6]
Postoperative and Rehabilitation Care
Stroke care is a multidisciplinary approach. All rehabilitation services should be involved including physical, occupational, and speech/cognitive therapies. Poststroke complications should be followed closely for prevention and management.
- Patients treated with tPA may have angioedema acutely. If there is life-threatening angioedema or laryngospasm, tPA should be stopped immediately.
- Neurological deterioration is worse within 72 and 96 hours after stroke in hemorrhagic transformation and malignant cerebral edema.
- Hydrocephalus may develop in posterior circulation strokes more than anterior circulation strokes. In this case, craniotomy and external ventricular drain (EVD) should be considered.
- Increased risk of venous thromboembolism includes pulmonary embolism and deep venous thrombosis (DVT) in the first months due to decreased mobilization. Patients in a hospital should be on chemical DVT prophylaxis if there is no contraindication like giving tPA in 24 hours or hemorrhagic transformation.
- Dysphagia should be addressed with percutaneous endoscopic gastrostomy tube placement before discharging the patient from the hospital if someone fails the swallowing tests with speech therapists.
- The risk for infections like pneumonia and urinary tract infection will be higher; however, there is no indication to use prophylactic antibiotics.
- Increased risk of seizures. There is no indication to use prophylactic antiepileptic drugs.
- Depression affects patients with CVA more in the first year. Fluoxetine helps for poststroke depression.
- Muscle relaxants may help with spasticity. If it is resistant, onabotulinumtoxinA injection is the next best step with oral medications.
- Decubitus ulcers may develop on bedbound patients. Changing the position of patients every 2 hours is beneficial.
- Increased mobility to prevent DVTs and deconditioning with family and physical and occupational therapy at the hospital, home, or nursing home.
Deterrence and Patient Education
"BEFAST" is a good and handy acronym to recognize common signs of a stroke, regardless of the etiology. Stroke is an emergency. Time is brain.
- Balance- Is there a sudden onset loss of balance or coordination?
- Eye- Is there a sudden onset blurred or double vision or any sudden onset, persistent vision problems?
- Face- When the person smiles, does one or both sides of the face hang limply?
- Arms- Ask the person to raise both arms. Does one side slope downward? Is there a sudden onset weakness/numbness on one side?
- Speech- Does the person have slurred or garbled speech? Can the patient repeat simple phrases?
- Time- Call 911 for immediate medical attention upon noticing one or more or these signs. Also, one should take note of when the symptoms began.
To help prevent strokes, one should:
- Monitor blood pressure
- Control cholesterol and blood sugar
- Get active and lose weight
- Eat healthily
- Stop smoking cigarettes
- Control obstructive sleep apnea
- Establish primary care to get medical attention.
Enhancing Healthcare Team Outcomes
Patients with a stroke are usually managed by an interprofessional team that includes the emergency department physician, neurologist. intensive care unit nurses, radiologists, physical therapists, occupational and speech therapists, and other specialists depending on the functional deficit. The key is to restore the patient to pre-stroke functioning levels, if possible. For patients with a minor stroke recovery is good but those who have gross neurological deficits at the time of admission usually require prolonged rehabilitation and there is often no guarantee of full recovery.[36]
(Click Image to Enlarge)

Figure 5 – An axial section on noncontrast CT head shows left PCA ischemic stroke and no hemorrhage.
Contributed by Okkes Kuybu, MD
(Click Image to Enlarge)

Stroke, Posterior Cerebral Artery
Contributed by Dr. Okkes KUYBU, M.D.
(Click Image to Enlarge)
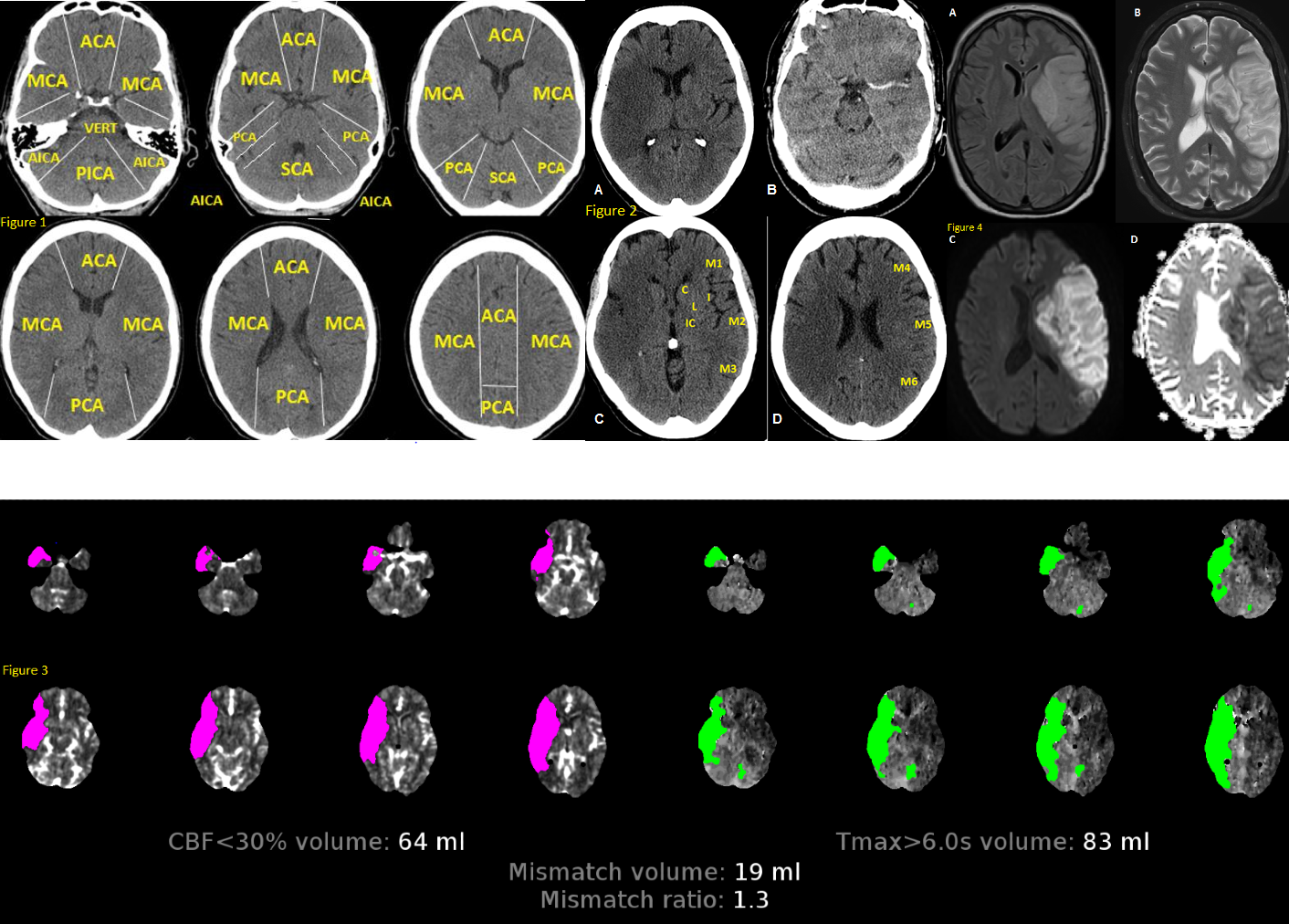
Fig 1. Anatomy of brain vascular territories. ACA: anterior cerebral artery; MCA: middle cerebral artery; PCA: posterior cerebral artery; AICA: anterior inferior cerebellar artery; PICA: posterior inferior cerebellar artery; SCA: superior cerebellar artery. Fig 2. Non-contrast CT shows loss of gray-white matter diffraction in the right MCA territory consistent with acute large right MCA infarction Fig 3. CTP in stroke imaging. The areas of increased MTT, TTP or Tmax and decreased CBV or CBF are considered as infarct core Fig 4. MRI in stroke. There is a large left MCA infarction. Infarction is hypersignal on FLAIR (A) and T2 (B) sequences. Also, there is a mass effect in favour of subacute infarction. The infarction shows “true” diffusion restriction: hyper signal on DWI (C) and hypo signal on ADC map (D).
Contributed by Omid Shafaat, M.D.