Anatomy, Abdomen and Pelvis, Prostate
- Article Author:
- Omesh Singh
- Article Editor:
- Srinivasa Rao Bolla
- Updated:
- 8/23/2020 8:33:19 PM
- For CME on this topic:
- Anatomy, Abdomen and Pelvis, Prostate CME
- PubMed Link:
- Anatomy, Abdomen and Pelvis, Prostate
Introduction
The prostate gland is situated in the true pelvis and plays a supportive role in the male reproductive system. Its principal purpose is to secrete alkaline solution protective for sperm in the acidic environment of the vagina. The fluid acts to balance the acidity of the vagina, which increases the overall lifespan of the sperm, allowing the greatest length of time to fertilize an egg successfully. The fluid also contains supportive proteins and enzymes that provide nourishment to sperm. The added volume of the prostatic fluid to the seminal fluid and sperm allow for easier mechanical propulsion through the urethra.
Structure and Function
The prostate is a dense fibromuscular gland. Its shape is like an inverted cone having a base above surrounding the neck of the urinary bladder, apex below situated on the external urethral sphincter.
Location: The prostate lies directly inferior to the bladder and wraps around the proximal urethra in the lesser pelvis. A fibrous capsule encloses the gland, with the nerves and vascular plexus which is further surrounded by a visceral layer of pelvic fascia.
Relations:
- Anteriorly, it is posterior to the pubic symphysis, separated by a pad of fat (retropubic fat) and venous plexus (prostatic venous plexus)
- Posteriorly it is in a close relationship to the rectum and is separated by fascia of Denonvilliers
- The external urethral sphincter muscle is beneath the prostate where it wraps around the urethra help to control ejaculatory and urinary flow
- On the lateral aspects, the gland is related to the levator ani muscle of the pelvic floor covered by endopelvic fascia
The prostate gland idivides anantomically into five lobes: anterior and posterior lobes, two lateral lobes, and one median lobe. This description is in many anatomical textbooks. In clinics, it is described as having two lateral lobes right and left and a median lobe.
The prostate gland is composed of histologically different zones; based on these, the gland divides into three anatomical zones.[1]
- The central zone forms the base of the gland that surrounds the ejaculatory ducts
- The peripheral zone is the largest zone making up 70% of the gland and surrounds most of the central zone and partially surrounds the distal part of the prostatic urethra
- The transition zone is a small glandular zone that surrounds a portion of the urethra between the urinary bladder and verumontanum
- There is an area denoted as the anterior fibromuscular stroma within the prostate; this area is not glandular, and contains mostly muscular and fibrous tissue and surrounds an inferior portion of the prostate called the apex
- Lastly, the prostate is encompassed by a fibrous layer called a capsule
Importantly, the prostate gland has multiple tubular structures passing within it, including the proximal urethra and two ejaculatory ducts. The ejaculatory ducts enter the prostate immediately as it emerges from the seminal vesicles. Both of these ducts travel from posterior and lateral to medial and inferior. They ultimately converge at the urethra within the prostate gland on an area called the seminal colliculus.
Embryology
The prostate gland starts to develop laterally as epithelial buds from the urogenital sinus wall. These buds branch into solid cords which canalize and form the ducts and acini. The surrounding urogenital sinus mesenchyme forms the interfascicular fibroblasts and the smooth muscle of the prostate.[2] With androgenic stimulation of the androgen receptor expressed in prostatic Mullerian mesenchyma, the prostate forms.[3] In development, androgen secretion by Leydig cells is the chief regulator of prostate growth.[4]
Blood Supply and Lymphatics
As the prostate gland shares a close anatomical relationship with the bladder, it also shares a portion of the bladder’s blood supply. The inferior vesical artery is the major blood supply for the prostate, and it also receives blood supply from the middle rectal and internal pudendal arteries.
Veins around the prostate form the prostatic plexus which drains into internal iliac veins. The prostate drains to the internal iliac lymph nodes and the sacral lymph nodes.
Nerves
The prostate gland receives innervation via the autonomic fibers from the inferior hypogastric plexus, receiving sympathetic input from the hypogastric nerve.[5] Parasympathetic inputs derive via the pelvic nerve.[5] Both the hypogastric and pelvic plexuses provide sensory inputs for the prostate.[5]
Surgical Considerations
Cases of severe benign prostatic hyperplasia that have failed multiple medical interventions can be treated with the transurethral resection of prostate (TURP) procedure. For this procedure, an instrument is inserted retrograde through the urethra at the tip of the penis. The device is then used to trim areas of the prostate gland to allow a larger canal for urine flow from the bladder. Short-term complications of transurethral resection include hematuria, postoperative hemoglobin decrease, blood transfusion, clot retention, recatheterization, urinary retention, dysuria, and urinary tract infection.[6] Long-term complications include urethral stricture, bladder neck contracture, stress urinary incontinence, reoperation, retrograde ejaculation, and erectile dysfunction.[6] Erectile dysfunction can occur due to damage to the pudendal nerve.[7]
Clinical Significance
Benign prostatic hyperplasia, prostate cancer, and prostatitis are the three most noteworthy clinical conditions that can arise.
Benign prostatic hyperplasia is primarily a urological condition that can narrow the urethra, or protrude into the bladder, causing obstruction to urine flow. It results from nodular enlargement of the gland, rather than diffuse enlargement.[8] The most common complaints arising from benign prostatic hyperplasia include increased urine frequency, nocturia, and weak stream.[8] This condition is mostly treated conservatively, and commonly with the use of an alpha-1 receptor blocker. These agents bind and antagonize alpha-1 receptors in the bladder neck and prostatic urethra, which decreases smooth muscle tone, allowing improved passage of urine in benign prostatic hyperplasia.[8] Another form of treatment is a 5-alpha-reductase inhibitor, which prevents the conversion of testosterone to dihydrotestosterone.[8] The elimination of dihydrotestosterone causes prostate atrophy, which decreases its overall size and helps to resolve the obstruction. Anti-muscarinic pharmacotherapy may be used as well to inhibit the contractions of the detrusor muscles within the bladder, helping to reduce urinary frequency and urgency.[8]
Prostate cancer usually occurs as an adenocarcinoma. Although not well understood, the occurrence of prostate cancer can be related to several things. These include family history, increased BMI, smoking history, and ionizing/UV radiation.[9] Prostate cancer can have similar symptoms to benign prostatic hyperplasia. However, a difference in presentation can be that of low back pain due to metastases. Prostate cancer can spread through venous channels that communicate with the venous channels of the lower lumbar vertebrae. Prostate-specific antigen (PSA) is a controversial marker of prostate cancer. It can be used to help clinical diagnosis of a recurrence of cancer. However, it should not be used as an initial predictor of cancer as BPH can cause these levels to rise as well. 5-Alpha-reductase inhibitors show correlations with an increase of high-grade cancers but have also been shown to reduce the overall cancer burden.[9]
Prostatitis is the result of bacteria that commonly cause urinary tract infections. This condition primarily presents as pain, as well as an array of urinary tract symptoms.[10] Prostatitis can be difficult to diagnose as bacteria can seldom be detected.[10] Treatment of this usually involves antibiotics that cover gram-negative species.
Most of the carcinomas (75%) develop in the peripheral zone, and BPH tends to appear in the transitional zone.[11]
(Click Image to Enlarge)
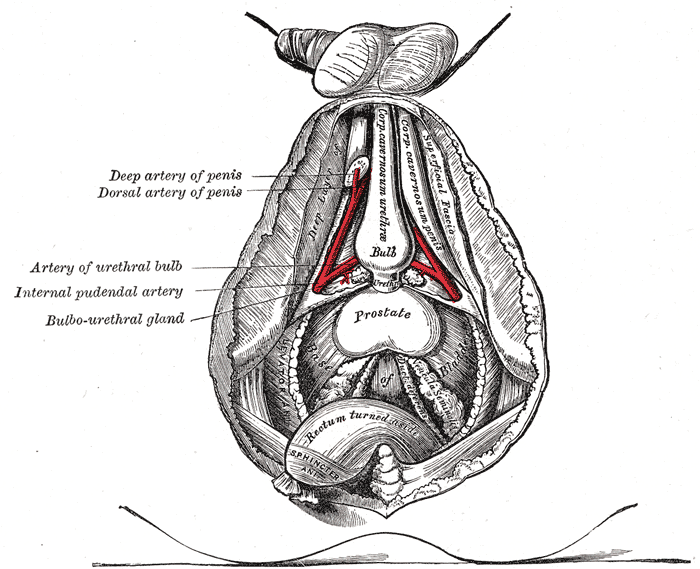
Arteries of the Penis, Deep and Dorsal Artery of the Penis, bulbourethral gland, Prostate, Artery of Urethral bulb, Internal pudendal artery, Bulbo-urethral gland,
Contributed by Gray's Anatomy Plates