Anatomy, Shoulder and Upper Limb, Forearm Radial Artery
- Article Author:
- Richard Marchese
- Article Editor:
- Zachary Geiger
- Updated:
- 8/15/2020 11:35:59 PM
- For CME on this topic:
- Anatomy, Shoulder and Upper Limb, Forearm Radial Artery CME
- PubMed Link:
- Anatomy, Shoulder and Upper Limb, Forearm Radial Artery
Introduction
The radial artery is one of two continuations of the brachial artery, the other being the ulnar artery. It supplies the anterior compartment of the forearm. The radial and ulnar arteries originate as a bifurcation of the axillary artery in the cubital fossa and serve as the major perforators to the forearm. Following its bifurcation, the radial artery runs along the lateral aspect of the forearm between the brachioradialis and flexor carpi radialis muscles.[1] Immediately proximal to the wrist, it splits into the superficial and deep palmar branches forming an anastomosis with the distal branches of the ulnar artery in the hand. The radial artery is quite superficial. It is easily palpated proximal to the wrist crease immediately lateral to the tendon of the flexor carpi radialis muscle.
Structure and Function
Arteries are composed of three layers:
Tunica Adventitia (Externa)
This is the outer covering of the artery. It is composed of connective tissue, collagen and elastic fibers which serve to allow distension of the wall during various pressure changes.[2]
Tunica Media
Located between the adventitia and intima. It is composed of circumferentially oriented smooth muscle and elastic fibers.
Tunica Intima
Inner layer which is composed of an elastic membrane and smooth endothelium.
Embryology
The initial proposal of embryological development of the upper limb as gradual sprouting of arterial trunks from a primitive axial artery was in 1933 by Singer. In 1995, Rodriquez-Baeza et al. proposed a method in which terminal branches of the superficial arterial segments of the brachial artery form anastomotic connections with the primitive axillary artery and regression patterns are responsible for the definitive arterial pattern.[3] Variations in these superficial branches may be responsible for anatomic variations of the axillary artery.
Blood Supply and Lymphatics
The branches of the radial artery are best organized based on their anatomical location; in the forearm, wrist, or hand. They are listed below based on their order of origination traveling distally along the upper extremity.
Forearm
Radial Recurrent artery – Originates below the origin of the radial artery, typical on the lateral aspect and travels proximally between the branches of the radial nerve, to anastomose with the radial collateral artery, a branch of the deep artery of the arm.
Muscular branches – distributed along the medial aspect of the radial artery as it travels distally and provides multiple perforators to muscles on the radial aspect of the forearm.
Palmar (volar) carpal branch – Arising near the distal aspect of the pronator quadratus. It travels across the carpal bones and anastomoses with the palmar carpal branch of the ulnar artery.
Superficial palmar branch – Originating from the medial aspect of the radial artery over the radial styloid it travels distally to anastomose with the terminal branches of the ulnar artery to form the superficial palmar arch.
Wrist
Dorsal carpal branch – Originates distal to the radial styloid and travels superficial over the scaphoid and anastomosis with the ulnar dorsal carpal branches to form the dorsal carpal arch. I
First dorsal metacarpal artery – Arises at the level of the first metacarpal as the radial artery enters the palmar aspect of the hands to form the deep palmar arch. It is composed of two arteries that supply the medial aspect of the first digit lateral aspect of the second digit.
Hand
Princeps pollicis artery (principal artery of the thumb) – Arises as the radial artery travels medially. It serves to supply the lateral aspect of the thumb and supplies the proper palmar digital arteries.
Radialis indicis artery (Radial artery of the index finger) – originates near the principal artery of the thumb and runs between the heads of the first dorsal interosseous muscle to supply the lateral aspect of the index finger.
Deep palmar arch – This is arterial anastomosis that is formed by the terminal components of the deep palmar branch of the ulnar artery and the radial artery.
Muscles
The radial artery supplies the posterolateral aspect of the forearm as well as vascular territories including the elbow joint, carpal bones, thumb and lateral index finger.
Physiologic Variants
The radial artery commonly occurs as a bifurcation in the antecubital fossa at the level of the radial neck and continues distally in the anterior forearm. Literature has documented that the brachial artery has multiple physiologic variants. These include a high origin from the axillary artery or the brachial artery, under the pronator teres or in some patients a congenital absence.[4][5][6]
Rodríguez-Niedenführ et al. refer to multiple terms used to refer to the concept of "high bifurcation."[4] Haladaj et al. reported the previous nomenclature for high bifurcation included: double brachial artery, high bifurcation of the brachial artery, the continuance of the superficial brachial artery as the radial artery. Haladaj et al. propose the term “brachial radial artery” to mean “ high origin of the radial artery.” A high origin of the radial artery was present in 9.2% of 120 cadavers; 18.1 % originated in the axillary cavity and the remaining 81.8% in the medial bicipital groove.[7]
Surgical Considerations
Radial Artery Laceration: Repair vs. Ligation
In 2015 Janice et al. compared operative to nonoperative approaches to forearm lacerations discovering that penetrating injury to the forearm must address for limb-threatening ischemia. In this setting, the restoration of blood flow via surgical management is necessary.[8] Though, given the rich anastomotic connections in the hand between the radial and ulnar artery, isolated laceration of either artery is not typically critical. In the presence of poor hemostasis, it is safe and acceptable to ligate a distal forearm artery as long as adequate perfusion exists at the palmar arch.[8] In the setting of complex lacerations involving both the radial and ulnar arteries, surgical repair is necessary.[8] It has been established that the magnitude of concomitant nerve injury, not arterial injury, is responsible for functional disability.[9]
Coronary Artery Bypass Graft (CABG)
Leonard et al. compared the efficiency of the radial artery and saphenous vein placement in the setting of CABG. Surgeons can use the radial artery as a conduit for CABG with excellent clinical outcomes.[10] Debs et al. showed the frequency of functional graft occlusion in radial arteries was 12.0% vs. 19.7% in saphenous vein placement.[11] Additionally, the incidence of complete graft occlusion in radial artery grafts were 8.9% vs. 18.6% in saphenous vein placement.[11]
Arteriovenous (AV) Fistulas
The radial artery has long found use as a site for the creation of arteriovenous fistulas for dialysis. In a paper by Jennings et al. reported that the proximal radial artery provided an excellent site for low-risk of dialysis-related steal syndrome.[12] While it has been recommended to create AV fistulas as far distal in the upper extremity as possible, Wu et al. documented low to moderate primary failure of proximal radial artery arteriovenous fistulas (PEAAVF) when selected as the primary site of PRAAVF formation; primary failure rate reached 12.3%.[13]
Carpal Tunnel Syndrome
Carpal tunnel syndrome is commonly due to thinking of the transverse carpal ligament, which leads to compression of the median nerve. Other causes include diabetes mellitus, tumors, and ganglia. With an incidence of less than 3%, an aberrant radial artery may lead to carpal tunnel syndrome.[14] When present, an aberrant radial artery arises from the main radial artery terminates at the wrist in the superficial palmar arch.[15]
Clinical Significance
Pulse
Palpation for the radial artery proximal to the wrist crease and immediately lateral to the tendon of flexor carpi radials muscle is a common site for medical professionals to document a patient’s pulse. Additionally, it can be palpated in the anatomical snuffbox as it crosses the lateral aspect of the wrist. The medial aspect of the snuffbox is the tendon of extensor pollicis brevis muscle. The lateral aspects are the tendons of the extensor pollicis longus and abductor pollicis longus muscles.[16]
Allen Test/Modified Allen Test
The Allen test, first described by Edgar Van Nuys Allen in 1929, is a medical test to determine the arterial blood flow to the hand. An alternative method, the modified Allen test, proposed by Irving Wright, is considered superior. The hand receives blood supply from both the radial and ulnar artery, which form an anastomosis in the hand. Therefore, if one supply is inadequate, the other can help ensure proper profusion to intrinsic hand muscles. Below is the technique for performing the modified Allen test.
The patient is asked to keep their arm flexed at the wrist. Next, they are asked first to clench their fist tightly or to open and close their hand repeatedly and then clench. The examiner then compresses the radial and ulnar arteries, simultaneously stopping blood flow to the hand. The elbow is then extended fully, avoiding overextension as it may lead to a false positive. The fist is then unclenched, and the hand should appear white. At this point, compression gets released from the ulnar artery, and the examiner observes the hand color. Hand color should return within 10 seconds. The test is repeated once again, with compression released from the radial rather than the ulnar artery.
In patients with proper arterial supply to the hand, color is restored promptly. Those with a compromised flow, from either artery, will have prolonged pallor following the release of arterial compression; this occurs secondary to an occlusion of the artery getting released, which continually reduces flow.
The modified Allen test is usable as a diagnostic tool to ensure proper arterial blood flow in patients undergoing vascular access or surgery in the hand. These procedures include arterial blood gases, cannulation, catheterization, or radial artery graft selection. Before any of these procedures, an Allen test/modified Allen test allows health care workers to determine if patients are at risk of developing hand ischemia.
(Click Image to Enlarge)
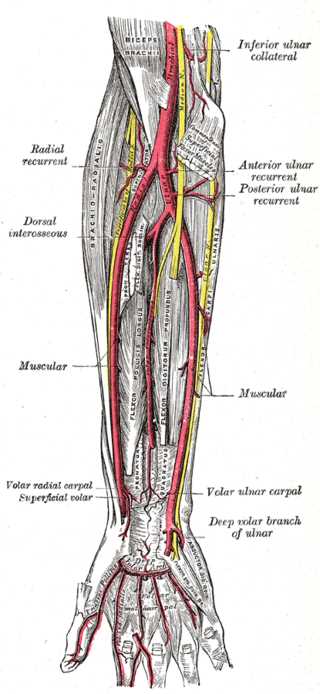
Deep Palmar Branch of the Ulnar Artery, Profunda Brachii Artery, Inferior ulnar collateral, Posterior Ulnar recurrent, Dorsal interosseous, Termination of Volar interosseous, Dorsal ulnar carpal, Dorsal radial Carpal, Radius, Ulnar
Contributed by Gray's Anatomy Plates