Diabetic Retinopathy
- Article Author:
- Unnati Shukla
- Article Editor:
- Koushik Tripathy
- Updated:
- 8/10/2020 9:37:52 PM
- For CME on this topic:
- Diabetic Retinopathy CME
- PubMed Link:
- Diabetic Retinopathy
Introduction
Diabetic retinopathy (DR) is a microvascular disorder occurring due to long term effects of diabetes, leading to vision-threatening damage to the retina, eventually leading to blindness. It is the most common cause of severe vision loss in adults of working age groups in the western world.[1] Early detection and timely intervention is the key to avoid blindness due to diabetic retinopathy. The number of patients with diabetic retinopathy in America is estimated to reach 16.0 million by 2050, with vision-threatening complications affecting around 3.4 million of them.[2] The usefulness of strict glycemic control was clearly seen in clinical trials like the UK Prospective Diabetes Study (UKPDS) and Diabetes Control and Complication Trial (DCCT).[3][4]
Uncontrolled diabetes can lead to many ocular disorders like cataract, glaucoma, ocular surface disorders, recurrent stye, non-arteritic anterior ischemic optic neuropathy, diabetic papillopathy, and diabetic retinopathy, out of which diabetic retinopathy is the most common and severe ocular complication.[5][6][7] Poor glycemic control, uncontrolled hypertension, dyslipidemia, nephropathy, male sex, and obesity are associated with worsening of diabetic retinopathy.[8][9]
Etiology
Diabetic retinopathy affects people with diagnosed or undiagnosed diabetes mellitus. The propensity of developing diabetic retinopathy is directly proportional to the age of the patient and duration of diabetes as well as with poor glycemic control and fluctuation blood pressure level.[10]
Risk factors for diabetic retinopathy can be classified into:[11]
- non-modifiable
- Puberty
- Pregnancy
- modifiable
- Hypertension
- Obesity
- Dyslipidemia
- Poor glycemic control
- Nephropathy
- Newer risk factors
- Inflammation
- Apolipoprotein
- Hormonal influence- Leptin and Adiponectin
- Vitamin D
- Oxidative stress
- Genetic factors
Epidemiology
Diabetic retinopathy is one of the major neurovascular complications of diabetes and is a leading cause of blindness in adults of working age group. According to the recent epidemiological data shared by the American Academy of Ophthalmology, the global burden of diabetes mellitus is 387 million, which is estimated to increase to 592 million by 2035. Ninety-three million people are globally affected by diabetic retinopathy. Prevalence of diabetic retinopathy is 77.3% in type 1 diabetes patients and 25.1% in type 2 diabetes patients, out of which approximately 25% to 30% are expected to develop vision-threatening diabetic macular edema.[12] Between 5% and 8% of patients with diabetic retinopathy need laser treatment.[13] As many as 0.5% of patients will require vitrectomy surgery.[14]
Pathophysiology
Chronic hyperglycemia is considered to be the primary pathogenic agent in DR (as described by UKPDS and DCCT).[4][3] Hyperglycemia leads to the activation of alternative pathways of glucose metabolism, including the polyol pathway, oxidative stress, protein kinase C activation, non-enzymatic protein glycation leading to advanced glycation endproducts (AGEs). The end result of these alternative pathways is the activation of cytokines along with the growth factors and vascular endothelial dysfunction, which eventually leads to increased vascular permeability and microvascular occlusion. Retinal ischemia, which occurs as a consequence of microvascular occlusion, leads to the formation of IRMA (intraretinal microvascular abnormalities) and neovascularization.[15][16]
In the polyol pathway, glucose is reduced to sorbitol by aldose reductase enzyme. The impermeability of sorbitol leads to its accumulation in all retinal cells leading to osmotic damage of the cells. Also, the use of NADPH (reduced nicotinamide adenine dinucleotide phosphate) during the reduction process leads to further oxidative damage.
Oxidative stress is a result of increased levels of reactive oxygen species (ROS), leading to cell and tissue damage.
Protein kinase C is involved in signal transduction. Its activation leads to basement membrane alterations along with vascular changes like increased vascular permeability, the release of angiogenic growth factors, vascular stasis, and capillary occlusion.
In non-enzymatic protein glycation, reducing sugars react with free amino acids of nucleic acids, proteins, and lipids leading to the formation of advanced glycation endproducts that are responsible for alteration in extracellular matrix proteins.
The morphological changes seen in small retinal vessels in DR include early loss of pericytes, basement membrane thickening, loss of endothelial cells, increased vascular permeability, platelet aggregation, leukostasis, and capillary dropout.[17][18]
Diabetic retinopathy does not only affect the microvessels of the retina but also the Muller cells, which are the primary glial cells of the retina. Functions of Müller cells are maintaining the structural integrity of the retina, regulation of the blood-retinal barrier and retinal blood flow, uptake and recycling of various neurotransmitters, retinoic acid compounds, and ions (such as potassium K), regulation of metabolism and supply of nutrients to the retina.[19] In diabetes, there is downregulation of Kir 4.1 channel because of which there is continued potassium uptake leading to swelling of Muller cells, which leads to Muller cell dysfunction.[20] Fluid accumulation inside the Muller cells is responsible for DME.[21][20]
Hyperglycemia leads to release of
- Growth factors[22], such as
- Vascular endothelial growth factor (VEGF),
- Pigment epithelium-derived factor (PEDF)[23],
- Platelet-derived growth factor(PDGF)[24]
- Basic fibroblast growth factor ( bFGF or FGF2)
- Insulin-like growth factor (IGF)
- Hepatocyte growth factor/scatter factor (HGF/SF)
- Placenta growth factor (PIGF)[25]
- Erythropoietin
- Angiopoietin-2
- Cytokines and Chemokines [26][27]including
- Interleukin-1β (IL-β),
- Interleukin-6 (IL-6),
- Tumor necrosis factor-α (TNF-α),
- Chemokine ligand-2 (CCL2)
Histopathology
Histologically diabetic retinopathy presents in the form of microangiopathy associated with vascular changes like focal capillary closure, dilatation of venules, hyalinization of arterioles, and capillary changes like basement membrane thickening, pericyte degeneration, focal outpouchings (microaneurysms). Capillary closure leads to cotton wool spots and ischemic areas, which lead to the development of IRMA (intraretinal microvascular abnormalities) and neovascularization, which is followed by fibrosis and contracture of the retina.[28][29] In diabetic retinopathy, the uptake of glutamate by Muller cells decreases, leading to glutamate toxicity.[30] Also, potassium conductance is decreased in proliferative diabetic retinopathy.[31]
History and Physical
Proper history taking should be done. This includes the duration of diabetes, type of diabetes mellitus, past glycemic control (HbA1C), medication, associated systemic disorders like obesity, kidney disease, hypertension, pregnancy, dyslipidemia, and nephropathy.
Patients might be asymptomatic in the early stages and might be discovered incidentally on fundus examination. As the disease progresses following symptoms might be seen- blurred vision, distorted vision, floaters, flashes, partial or total loss of vision, poor night vision, and impaired color vision in rare case scenarios.
Signs seen in diabetic retinopathy on fundus examination include:[32]
Microaneurysms:
- Focal saccular dilatation of the capillary wall
- Are located in the inner nuclear layer
- Are the earliest clinically detectable lesions
- Clinically identified by ophthalmoscopy as tiny, round, red dots with a sharp regular margin
- A diameter of 15- 60 µm (less than 125 µm). Microaneurysms with a diameter of less than 30 µm may not be detectable clinically.
- Initially appear temporal to the fovea
- May disappear with time
- Microaneurysms are differentiated from dot hemorrhages by FFA (fundus fluorescein angiogram) wherein microaneurysms show tiny hyperfluorescent points whereas dot hemorrhages show blocked fluorescence. Dot hemorrhages are clinically larger and may have an irregular margin.
Hemorrhages:
Weakened capillary wall ruptures leading to intraretinal dot hemorrhages. Superficial or flame-shaped hemorrhages arises from the precapillary arterioles located in the retinal nerve fiber layer. Deep hemorrhages or dot and blot hemorrhages are located in the inner nuclear and outer plexiform layers of the retina.
Hard exudates:
They are composed of lipoprotein and lipid-filled macrophages located in the outer plexiform layer. They develop at the junction of the edematous and non-edematous retina.
Cotton wool spots/soft exudates:
They are located in the retinal nerve fiber layer (axoplasmic debris) and represent focal infarcts of the precapillary arterioles.
IRMA (intraretinal microvascular abnormalities):
IRMA’s are intercommunications between retinal arteriole and venules, which bypass the capillaries and are seen near the areas of capillary closure. IRMA’s are intraretinal in location, do not cross the major vessels, and do no leak on fluorescein angiography.
Venous changes:
- Dilatation
- Looping
- Beading
- Sausage-like segmentation
Arterial changes:
- Peripheral narrowing
- Silver-wiring
- Obliteration
Neovascularization:
Neovascularization (new vessels) at the disc (NVD)- neovascularization at or within one disc diameter of the optic disc
Neovascularization elsewhere (NVE)- new vessels away from one disc diameter of the optic disc.
Neovascularization of Iris- It is a marker of poor prognosis and is associated with the propensity to develop neovascular glaucoma.
Early treatment diabetic retinopathy study (ETDRS) classification of diabetic retinopathy:[33][34]
Nonproliferative Diabetic Retinopathy
- No retinopathy: No retinal lesions
- Very mild NPDR: Microaneurysms only
- Mild NPDR: A few microaneurysms, retinal hemorrhage & hard exudates
- Moderate NPDR: Retinal hemorrhages (about 20 medium-large per quadrant) in 1-3 quadrant + cotton wool spots (between the grades mild and severe NPDR)
- Severe NPDR: fulfilling one rule of 4-2-1 rule.
- 4-2-1 rule
- Severe hemorrhages in all four quadrant
- Venous beading in 2 or more quadrants
- Moderate IRMA in 1 or more quadrants
- 4-2-1 rule
- Very Severe NPDR: fulfilling two or more rules of 4-2-1 rule.
Proliferative Diabetic Retinopathy
- Mild to moderate PDR- NVD or NVE insufficient to meet high-risk characteristics
- High risk PDR-
- NVD greater than ETDRS standard photograph 10A (about 1/3 disc area).
- Any NVD with vitreous hemorrhage.
- NVE greater than 1/2 disc area with vitreous hemorrhage.
Advanced Diabetic Eye Disease - End-stage vision-threatening complication of diabetic retinopathy in patients in whom the treatment is inadequate or unsuccessful. It may present as pre-retinal or intragel hemorrhage, tractional retinal detachment, or rubeosis iridis.
Diabetic Macular Edema (DME)- it can be classified into the following groups
- Focal exudative and diffuse exudative maculopathy
- Ischemic and non- ischemic maculopathy
- Tractional and non-tractional maculopathy
- Center involving macular edema and non-center involving macular edema
ETDRS classification of Clinically significant macular edema (CSME)[35][36]
- Retinal edema within 500 µm of the center of the fovea
- Hard exudates within 500 µm of the center of the fovea if associated with adjacent retinal thickening (which may be outside the 500 µm limit)
- Retinal edema one disc area (1500 µm) or larger any part of which is within one disc diameter of the center of the fovea
OCT (optical coherence tomography) classification of diabetic macular edema
- Sponge-like thickening of retinal layers
- Large cystoid spaces
- Serous detachment of the retina
- Tractional detachment of the fovea
- Taut posterior hyaloid membrane.
International Clinical Diabetic Retinopathy Disease Severity Scale:[37]
- No apparent retinopathy-No abnormality
- Mild NPDR- Microaneurysms only
- Moderate NPDR -More than just microaneurysms and less than severe disease
- Severe NPDR -No signs of PDR and any of the following:
- 20 intraretinal hemorrhages in each of the 4 quadrants
- Venous beading in ≥2 quadrants
- Prominent IRMA ≥1 quadrant
- PDR - One or more of the following:
- Neovascularization
- Vitreous or pre-retinal hemorrhage
With regards to Diabetic macular edema, the presence or absence of macular edema should be noted. It can further be classified into mild, moderate, and severe based on the distance of thickening and hard exudates from the center of the fovea.
Mild DME: The retinal thickening or hard exudates located far from the center of the fovea
Moderate DME: Retinal thickening or hard exudates approaching the center of the macula but not involving the center
Severe DME: Hard exudate and thickening involving the center of the fovea
Evaluation
Laboratory Examination
The following are the diabetic markers mandatory in all the patients getting screened for diabetic retinopathy.
- Fasting blood Glucose- The fasting blood glucose level of less than 110 mg/dl is normal. A fasting blood sugar (FBS) level of 110-125 mg/dl is considered prediabetes. FBS of more than 126 mg/dl, in at least two samples, denotes diabetes.[38]
- Postprandial blood glucose level after 2 hours- in 0-50 years is<140 mg/dl; 50-60 years <150 mg/dl;60 years and older <160mg/dl.[39]
- HbA1C (glycosylated hemoglobin)- The normal range of HbA1c is between 4% to 5.6%. Levels between 5.7% and 6.4% denote high chances of having diabetes. Levels of more than 6.5 % denote diabetes.[40]
Diabetes affects almost all the major organs of the body. Hence a thorough systemic examination should be done to rule out any diabetic complication. Especially Kidney function test, Cardiac function test, liver function test, thyroid markers, a neurological examination should be carried out in each and every patient on presentation. For this, a multispecialty approach is required.
Ocular Examination
On presentation, the patient should be thoroughly tested for:-
- Visual acuity,
- IOP measurement,
- Gonioscopy (for neovascularization of iris/angles and for raised intraocular pressure/IOP),
- Slit-lamp examination (to rule out other ocular manifestations of diabetes mellitus),
- Dilated fundus examination with +78 or +90 D lens for posterior pole (on slit lamp) and with +20 or +28 D lens for detailed peripheral examination (with an indirect ophthalmoscope) and diabetic retinopathy grading should be done.
The following additional posterior segment investigations should be done for confirmation of the diagnosis of diabetic retinopathy.[41]
Fundus Photography
- For documentation and record purposes.
- It is a very helpful tool for patient education, as well.
Fundus Fluorescein Angiography (FFA)
- For the diagnosis of ischemic maculopathy.
- To locate capillary dropout areas.
- To differentiate IRMA from neovascularization.
- To differentiate disc collaterals from disc neovascularization.
- To reveal occult new vessels that could not be detected on clinical examination
- To find out the cause of unexplained visual loss.
Optical Coherence Tomography (OCT):-
- to evaluate retinal thickening
- assessment and monitoring of edema after initiation of treatment
- very helpful marker to plan for the next sitting of intravitreal injections.
- to diagnose Vitreomacular traction (VMT) and the epiretinal membrane (ERM) which might require surgery (pars plans vitrectomy)
Ultrasonography (B Scan)
- it is a very useful tool in hazy media for diagnosis of
- Vitreous hemorrhage
- Tractional retinal detachment
- Subhyaloid hemorrhage
- Posterior vitreous detachment
Optical Coherence Tomography Angiography (OCTA)
OCTA employs motion contrast imaging to retinal blood flow, generating images that are similar to fluorescein angiography without injecting the dye invasively.
- Provides detailed information of the retinal vasculature
- Helpful for demarcation of foveal avascular zone helping to find out foveal ischemia
- Accurate detection of even mild IRMA
- To delineate capillary drop out areas.
- Vascular signs like looping, beading, dilatation can very well be appreciated on OCTA.
- The earliest detection of microvascular changes (before the visibility of microaneurysm).
- Especially useful in patients with kidney disease and patients prone to an anaphylactic reaction to the dyes.
Treatment / Management
General Systemic Control of Diabetes
- Strict metabolic control of diabetes.
- HbA1C levels should be kept under 6.5%.[42]
- Lifestyle modifications like routine exercises and proper diabetic food diet.
- Patients should visit diabetologists for proper follow-up visits and should take timely antidiabetic medications.
- Other systemic ailments like hypertension, dyslipidemia, hypoproteinemia, anemia, nephropathy, neuropathy, cardiac ailments, and others should also be taken care of by respective medications.
(a) Management of Non-Proliferative Diabetic Retinopathy
Strict glycemic control and strict compliance of patients towards antidiabetic medication is the key to manage a case of NPDR. Stress should be on proper systemic control of diabetes mellitus, keeping a watch on the progression of ocular findings. Associated comorbidities should be taken care of. A detailed systemic investigation by a physician or an endocrinologist should be done to rule out any other systemic side-effects of diabetes mellitus.
- Very mild NPDR- followup every yearly.
- Mild to moderate NPDR - followup 6-12 monthly.16% cases of mild NPDR and 23% cases of moderate NPDR progress to proliferative stages within four years.[37]
- Severe to Very Severe NPDR- Close followup within 2-4 months. 50% of severe NPDR and 75% of cases of very severe NPDR progress to PDR within one year.[37]
(b) Management of Diabetic Macular Edema
Center involving diabetic macular edema -nowadays, anti-VEGF agents have become the first line of treatment for center involving diabetic macular edema. Bevacizumab, Ranibizumab, and aflibercept have shown to have beneficial effects in patients with baseline better visual acuity. Aflibercept is shown to have better visual outcomes in patients with worse baseline visual acuity on presentation.[43] Recently, Aflibercept and Ranibizumab have received FDA approval for use in diabetic retinopathy associated with Macular edema.[44] Intravitreal steroid implants also are used in recalcitrant cases.[45]
Non-center involving macula - Focal or Grid laser-guided by ETDRS is the treatment of choice.
Nowadays, in the era of Anti- VEGF medications, laser treatment is usually avoided in the center involving macular edema. It may be added as adjuvant therapy in patients not responding to anti-VEGF therapy alone. From the results of the DRCR network (diabetic retinopathy clinical research), it was found that monthly loading doses of Ranibizumab followed by pro re nata or PRN schedule (as and when needed) have better results in center involving macular edema than single therapy with laser or steroids alone. As stated by ETDRS, laser helped in halting the progression of moderate visual loss, but it did not improve the visual acuity. Bevacizumab intravitreal injection is also effective in the center involving DME, but it is not FDA approved. Hence it is available only as an off label use. Cluster endophthalmitis due to fake drugs or other reasons is another concern.[46] DRCR network also studied the role of aflibercept in DME, and it was found to be useful in patients with initial worse visual acuity (Protocol T of DRCR.net).[43] Other notable studies other than the DRCR network on intravitreal Anti-VEGF injections included RISE, RIDE, READ, RESTORE, BOLT, and RESOLVE.
Doses of commonly used intravitreal injections:-
Bevacizumab- 1.25mg/0.05 ml (PACORES, DRCR.net PROTOCOL H, BOLT, READ-2)[47][48][49][50][51][50][48][47]
Ranibizumab - 0.5 mg or 0.3 mg /0.05 ml(RESOLVE, DRCR.net PROTOCOL I, RESTORE, RISE/RIDE[52][53])[54][55][56][55][54]
Aflibercept -2 mg/0.05 ml (DA VINCI, VISTA/VIVID, DRCR.net PROTOCOL T)[57][58][59][58][57]
Pegaptanib- 0.3mg/0.9 ml [not FDA approved for this indication](Cunningham et al, Sultan et al)[60][61][60]
Long-acting corticosteroid implants like Dexamethasone implant (OZURDEX), the fluocinolone acetonide implants (RETISERT and ILUVIEN) are also used in Diabetic macular edema. Though they are not considered as the first line of treatment. They are reserved for cases not responding to multiple injections of Anti-VEGF medications (according to protocol U of DRCR.net).[62] Their main advantage is long term control of inflammation and lesser frequency of administration. The high cost is also one of the factors for its limited use. Intravitreal injections of triamcinolone are not FDA approved, have poorer results, and is linked with more complications than anti-VEGF medications. Glaucoma is an important side effect of intravitreal steroids.
Tractional diabetic macular edema can occur because of VMT (Vitreomacular traction) or ERM (Epiretinal membrane), Vitrectomy surgery should be considered. Intravitreal injections might worsen the tractional component. Laser spots, too, should be given away from the tractional area to avoid further worsening.
Refractory Diabetic macular edema- macular edema not responding to multiple injections of anti-VEGF and, at least, one sitting of laser is considered to be refractory ones.[63] A possible approach to such cases include evaluating systemic control, higher dosing or frequency of anti-VEGF medications, use of steroid implants (according to protocol U of DRCR.net), rechecking of the diagnosis, ruling out any unfavorable anatomical causes, and ultrawide field angiography to look for extreme peripheral ischemic areas and to laser as far in the periphery as possible.[64][62][65][64]
Ischemic type of diabetic macular edema is associated with poor visual prognosis. Laser therapy and anti-VEGF are relative contraindications in this condition.[66] The patient can be considered for an extreme peripheral laser to kill out the ischemic areas responsible for VEGF release.[67] Steroid implants could be tried. However, the prognosis is guarded despite all the measures.[66]
(c) Treatment of Proliferative Diabetic Retinopathy (PDR)[68]
Panretinal photocoagulation (PRP) is considered to be the standard treatment of proliferative diabetic retinopathy for ages. But because of its destructive properties, intense research was done to find an alternative non-destructive mode of management of diabetic retinopathy. Various studies evaluated the role of intravitreal anti-VEGF injections in PDR cases. Because of the limited half-life of these injections, repeated injections at timely intervals become mandatory. Hence cost-effectivity of this regime is questionable. A concoction of intravitreal injection and pan-retinal photocoagulation depending on the severity of the disease and taking into account the presence or absence of macular edema helps in the proper management of diabetic retinopathy patients.
- Non-high-risk PDR without DME - careful 2-4 months followup and immediate pan-retinal photocoagulation if high-risk PDR occurs. Some physicians perform PRP in all PDR cases.
- High-risk PDR without macular edema- pan-retinal photocoagulation should be initiated.[69]
- PDR with CSME- combined intravitreal anti-VEGF injections and PRP sessions should be considered.
- High-risk PDR in which complete photocoagulation is not possible- alternatives like cryopexy or vitrectomy should be considered.[69]
In Protocol S of DRCR.net, a comparison of safety and efficacy of PRP to intravitreal injection of 0.5 mg ranibizumab was studied. The primary outcome of protocol S Ranibizumab 0.5 mg was non-inferior to PRP. Hence there are chances that Ranibizumab might compete with PRP to be the first line of management in the near future. High cost, repeated injection, multiple followup visits, distortion of the vitreous anatomy, and physiology because of the repeated injections, chances of endophthalmitis, tachyphylaxis are some of the hindering factors though.[70]
(d)Treatment of Advanced Diabetic Eye Disease
Prognosis is guarded in patients of advanced diabetic eye disease. Persistent vitreous hemorrhage can initially be given the trial of intravitreal injection of anti-VEGF agent following which if the hemorrhage resolves, then scattered pan-retinal photocoagulation in the visible areas can be tried.[71] Ultrasnogram must exclude retinal traction if such an approach is considered.
If the hemorrhage does not resolve with the above management, pars plana vitrectomy should be considered. Also, in cases presenting with tractional retinal detachment, vitrectomy is the treatment of choice.
Indication of Vitrectomy in diabetic patients include:
- Non-clearing vitreous hemorrhage (vitreous/subhyaloid/pre-macular)
- Tractional retinal detachment with macula off
- Combined tractional with rhegmatogenous retinal detachment
- Anterior segment neovascularization with the invisibility of the posterior segment
- Ghost cell glaucoma
- Thick epiretinal membrane
- Vitreomacular traction
In vitrectomy surgery, three pars plana ports are made, one for the infusion line, one for the light pipe, and the third one for the microinstruments. A fourth port can be made if a chandelier light source is used in cases of bimanual vitrectomy.[72] Core vitrectomy with guarded PVD (posterior vitreous detachment) induction is done. The peripheral vitreous is shaved. All bleeders are cauterized. All tractional components are removed. Fluid- Air exchange is done. If required, ERM peeling with or without ILM (internal limiting membrane) peeling is done with due precautions.360 degree pan-retinal endophotocoagulation is done. At the end of the surgery, tamponade in the form of air, fluid, gases (C3F8, SF6), or silicone oil, can be injected.
In cases of rubeosis iridis, in the early phases, pan-retinal photocoagulation with or without anti-VEGF medication might be helpful. In the advanced stages, the new vessels lead to fibrosis and contracture, leading to permanent distortion of the angles leading to refractory glaucoma, which might eventually require glaucoma drainage implant). The prognosis is, however, poor in such cases. Painful blind eyes may need diode laser cyclophotocoagulation or cyclocryotherapy.
(d)Treatment of Diabetic Retinopathy (without DME)
This is an FDA approved indication of ranibizumab and aflibercept, which can reduce the severity of diabetic retinopathy.
Differential Diagnosis
The differential diagnosis of diabetic macular edema includes:[73]
- Hypertensive retinopathy
- Central retinal vein occlusion
- Branch retinal vein occlusion
- Irvine glass syndrome
- Post uveitic macular edema
- Ruptured macroaneursym
- Macular edema secondary to epiretinal membrane
- Choroidal neovascular membrane
- Pseudophakic cystoid macular edema
The diseases which can be mistaken as diabetic retinopathy based on the general fundus appearance includes:
- Central retinal vein occlusion[74]
- Hypertensive retinopathy[75]
- Sickle cell retinopathy[76]
- Terson syndrome[77]
- Ocular ischemic syndrome[78]
- Branch retinal vein occlusion[79]
- Hemiretinal vein occlusion[80]
- Valsalva retinopathy[81]
- Post-traumatic retinal bleed[82]
- Retinal macroaneurysm[83]
- Retinopathy in thalassemia[84]
Prognosis
Prognosis of diabetic retinopathy depends on the duration of diabetes, glycemic control, associated comorbid conditions, compliance of the patient to the appropriate line of treatment.[85][86] Proper patient counseling is needed about his/ her retinal condition and making patients aware that delay in proper followup could lead to permanent, irreversible loss of vision. Initial stages of diabetic retinopathy are reversible if proper glycemic control is achieved. Many patients with diabetic macular edema require long term support of repeated injections of intravitreal anti-VEGF medications. Patients treated with pan-retinal photocoagulation may require additional supplementation of anti-VEGF medications if there is persistent macular edema and neovascularization. Once there is tractional macular detachment for a longer duration of time, then the visual prognosis is usually guarded as the macular anatomy is markedly distorted.
OCT biomarkers of prognosis of diabetic retinopathy include refractile bodies, disorganization of inner layers of the retina (DRIL), disruption of outer layers of the retina (DORL), macular thickness, choroidal thickness, epiretinal membrane, vitreomacular adhesions, subretinal fluid, and integrity of ellipsoid zone.[41][87]
Complications
Vision threatening complications associated with poorly controlled diabetic retinopathy include diabetic macular edema, tractional retinal detachment, and vitreous hemorrhage as a late sequela of proliferative diabetic retinopathy.[88][89]
Management of Diabetic retinopathy with Anti-VEGF therapy, Laser photocoagulation, or vitrectomy surgery is also not free of complications.
Complications Related to Anti-VEGF Medications
- IOP spike
- Cataract formation
- Iatrogenic retinal/posterior capsular tear
- Vitreous hemorrhage
- Rhegmatogenous Retinal detachment
- Worsening of traction over the macula if given in patients with tractional retinal detachment
Complications Related to Laser Photocoagulation
- Vitreous hemorrhage
- Exudative retinal detachment and choroidal detachment if too many laser shots are given in a single sitting
- Reduction of contrast sensitivity, peripheral vision, and night vision after pan-retinal photocoagulation,
- Permanent scotomas in the visual field.
- Worsening of preexisting macular edema or development of macular edema after laser/PRP
- Chances of worsening of optic disc pallor
Complications Related to Vitrectomy
- Cataract formation
- IOP spike because of gas or oil tamponade
- Iatrogenic secondary tears leading to rhegmatogenous retinal detachment
- In chronic macular edema, the macular roof is very thin, so there are chances of deroofing at the macular region leading to a macular hole.
Postoperative and Rehabilitation Care
Laser photocoagulation is performed as an OPD (outpatient department) procedure. No additional care is required for it. Just maintenance of proper glycemic control and taking care of other associated systemic illness are necessary. There are chances of worsening of macular edema and moderate reduction of vision after panretinal photocoagulation (PRP). If that happens, the patient should report to the retinal surgeon for documentation and for planning a further line of management.
It is common to have an acute spike of IOP after intravitreal injections for a few hours. It usually returns to normal within 3-6 hours. It may be prudent to routinely use a single tablet of acetazolamide 250mg stat after intravitreal injection. After intravitreal injections, patients should be called for followup the next day, then according to the stability of the ocular condition, followup at regular intervals should be planned. Sequential OCT and/or OCTA parameters are assessed in each followup visit, and depending on their findings, further management with repeat injections, observation, and/or switching to laser /vitrectomy surgery is planned.
Post- Surgery Care
After surgery, the eye is patched. After the patch is removed, the eye is cleaned, and topical administration of medications like antibiotics with steroid eye-drops and cycloplegic eye-drops are started. After injecting gases like sf6/c3f8 or silicone oil, there are chances of IOP spike post-operatively, which needs to be managed with appropriate antiglaucoma medications. Patients can then be called for regular, timely followups to screen the post-operative outcomes. If silicone oil tamponade is done, the patient should be explained the need for a mandatory second surgery for removal of oil.
Deterrence and Patient Education
The American Academy of Ophthalmology's current recommendation states that people with diabetes mellitus type 1 should have yearly screening for diabetic retinopathy starting at five years after the onset of diabetes, and patients with diabetes mellitus type 2 should have fundus evaluation at the time of diagnosis and annually thereafter.[90][91]
The patient should be counseled properly regarding the prognosis of diabetic retinopathy. Early diagnosis, management, and follow-up visits at timely intervals, depending on the stage of presentation of diabetic retinopathy, are mandatory. Systemic dysregulation of diabetes can lead to an exponential worsening of diabetic retinopathy. Lifestyle modification should be done along with proper systemic as well as topical medications to halt the progression of diabetic retinopathy.
Enhancing Healthcare Team Outcomes
Any patient presenting with diabetic retinopathy should not receive treatment solely by an ophthalmologist in isolation. It requires a multispecialty evaluation by an endocrinologist, nephrologist, cardiologist, and neurologist. Interprofessional communication can lead to better patient management. The patient will most often present to the primary health care provider or nurse practitioner, and these professionals should be aware of the condition as it is treatable. Prompt referral to an ophthalmologist is necessary. These patients can then be followed by their primary clinicians and should ensure correct dosing on the medication management aspect of the condition.
Nursing will be the first department to come in contact with the patients on followup and can assess the treatment progress as well as evaluate the compliance with both medication and lifestyle measures, and report any issue to the primary care physician. This collaborative, interprofessional approach to care can ensure optimal patient outcomes.
(Click Image to Enlarge)
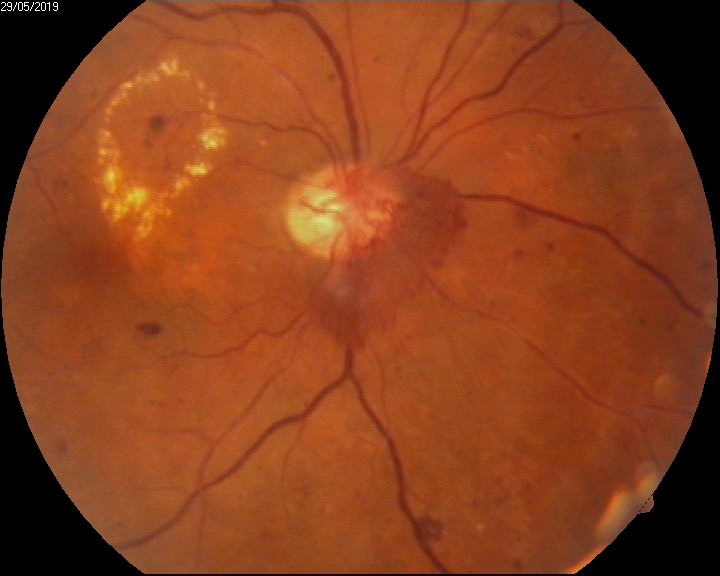
diabetic retinopathy- neovascularisation of disc (NVD)
Contributed by Unnati Shukla, MS,DNB,MNAMS,FVRS,PhD Scholar