Neurosurgery, Sensory Homunculus
- Article Author:
- John Nguyen
- Article Editor:
- Hieu Duong
- Updated:
- 7/31/2020 2:56:53 PM
- For CME on this topic:
- Neurosurgery, Sensory Homunculus CME
- PubMed Link:
- Neurosurgery, Sensory Homunculus
Introduction
The word "homunculus" means little man in Latin. But in neuroanatomy, the cortical homunculus represents either the motor or the sensory distribution along the cerebral cortex of the brain. The motor homunculus is a topographic representation of the body parts and its correspondents along the precentral gyrus of the frontal lobe. While the sensory homunculus is a topographic representation of the body parts along the postcentral gyrus of the parietal lobe.
Structure and Function
The sensory homunculus is a topographic representation of the sensory distribution of the body found in the cerebral cortex. This topograph usually has body parts illustrated along the surface of the postcentral gyrus of the parietal lobe. The topography of the sensory homunculus corresponds to the contralateral side of the body. Starting from the medial aspect of the postcentral gyrus, this area corresponds to the sensory territory of the genitals and lower extremities. Moving more laterally along the postcentral gyrus, the superior to superolateral regions of the gyrus corresponds to the neck, shoulder, and torso. While along the lateral side of the postcentral gyrus, this region corresponds to the upper extremity and hand. The inferolateral region of the postcentral gyrus corresponds to the facial and bulbar structures. Interestingly, the face is the structure that takes up the most area of the sensory homunculus.[1][2][3][4][5]
The sensory homunculus is a map along the cerebral cortex of where each part of the body is processed. The sensations occur all along the body. The impulses from the body will be sent into the spinal cord and eventually back to the brain to be processed. While the trigeminal nerve carries the face's sensations. The thalamus processes all these sensory impulses, and then the thalamus will send it to the cerebral cortex. The final destination of the sensory impulses is along the postcentral gyrus. This sensory map is what the sensory homunculus illustrates.
Embryology
During embryology, the nervous system is developed from the ectodermal germ layer. In the beginning, the notochord is beneath the ectoderm and induces the ectoderm to differentiate into the neuroectoderm and the neural plate. It is the neural plate that will further differentiate into the neural tube and the neural crest cells. The neural tube is responsible for developing the central nervous system. While the neural crest is responsible for the development of the peripheral nervous system.
The neural tube will further differentiate into the prosencephalon, mesencephalon, and the rhombencephalon. First, the prosencephalon is further divided into the telencephalon and the diencephalon. The telencephalon will develop into the cerebral hemispheres, basal ganglia, and the lateral ventricles. This makes the telencephalon the origin of the postcentral gyrus. While the diencephalon will develop into the thalamus, hypothalamus, and the third ventricle. Secondly, the mesencephalon will develop into the midbrain and the cerebral aqueduct. Lastly, the rhombencephalon will further differentiate into the metencephalon and the myelencephalon. The metencephalin later develops into the pons, cerebellum, and the upper part of the fourth ventricle. Finally, the myelencephalon will develop into the medulla and the lower part of the fourth ventricle.
Blood Supply and Lymphatics
Arterial
The perfusion of the postcentral gyrus is predominantly from the middle and anterior cerebral artery. The middle and anterior cerebral artery arises from the internal carotid artery. Once the internal carotid artery reaches the brain, it splits into the middle cerebral artery and the anterior cerebral artery. The middle cerebral artery ascends the brain between the temporal and the frontal lobe. This path corresponds to the perfusion territory of the middle cerebral artery. The middle cerebral artery will perfuse the inferior and lateral region of the postcentral gyrus, which corresponds to the face and hand part of the homunculus. As for the anterior cerebral artery, it will ascend between the two frontal lobes. The anterior cerebral artery will go on and perfuse the medial and superior region of the postcentral gyrus. The medial and superior part of the postcentral gyrus corresponds to the legs and the genitals respectively on the homunculus. The region of the postcentral gyrus that corresponds to the neck, shoulders, and torso is considered the watershed area. The watershed region received perfusion at the point where the distal ends of the anterior and middle cerebral arteries meet.
Venous
The venous blood and cerebral spinal fluid in the brain drain into the dural venous sinuses. The dural sinuses derive from the folds of the meninges. The dura sinuses are unique structures that drain venous blood similar to veins, but dura sinuses lack valves. The venous blood from the dura sinuses drains towards the internal jugular veins. Then the internal jugular veins merge with the subclavian vein to form the brachiocephalic vein. Both the left and right brachiocephalic veins join to form the superior vena cava. The venous blood from the superior vena cava empties into the right atrium of the heart.
Lymphatics
The lymphatic system of the brain was once believed to be nonexistent. But in recent findings, researchers found that the lymphatic system of the brain is embedded in the dura mater layer of the meninges. The lymph drains from the dura mater towards the cervical lymph nodes. The lymph from the cervical lymph nodes will either drain into the right lymphatic duct if it's on the right side of the head or the thoracic duct if it's on the left side of the head. Both the right lymphatic duct and the thoracic duct will drain back into the central circulation.[6][7][8]
Nerves
The sensory homunculus does not contain nerves. But the sensory impulses from the body's sensory receptors such as the free nerve endings, Meissner corpuscles, Pacinian corpuscles, Merkel disc, and Ruffini corpuscles are processed in the thalamus and sent to the postcentral gyrus of the parietal lobe. In contrast, the sensory of the face follows the distribution of the trigeminal nerve (CN V).
Sensory Receptors and Senses
- Free nerve endings - pain and temperature
- Meissner corpuscles - fine/light touch and position sense
- Pacinian corpuscles - vibration and pressure
- Merkel discs - pressure, deep static touch, and position sense
- Ruffini corpuscles - pressure, slippage of objects along the surface of the skin, and joint angle change
Spinal Cord Tract
The free nerve endings are responsible for sensing pain and temperature. The sensation of pain and temperature gets transmitted to the brain via the spinothalamic tract in the spinal cord, while transmissions from the Meissner corpuscles, Pacinian corpuscles, Merkel disc, and Ruffini corpuscles sensations travel to the brain via the dorsal column in the spinal cord. Once these tracts arrive in the brain, they synapse in the ventral posterolateral nucleus of the thalamus. Finally, the thalamus will send the impulse to the postcentral gyrus of the parietal lobe (sensory cortex).[9][10][11]
The sensory receptors on the face will send impulses toward the brain following the distribution of the trigeminal nerve. The impulses from the face will synapse in the ventral posteromedial nucleus of the thalamus. Finally, these impulses will get transmitted to the sensory cortex in the brain.
Muscles
The sensory homunculus does not involve muscles directly. But muscles are indirectly involved due to the sensory receptors that sense muscle position and changes in muscle length. The sensory homunculus is mainly a topographic representation of body structures along the postcentral gyrus of the parietal lobe.
Physiologic Variants
The contour and shape of the postcentral gyrus may vary in different individuals, but the sensory homunculus representation along the postcentral gyrus is relatively constant.
Surgical Considerations
Brain surgeries that involve the circle of Willis could cause damage to the sensory distribution of the homunculus due to the blood supply to this region are from the middle and anterior cerebral arteries. The damage to the blood supply would involve the postcentral gyrus, but not isolated to this gyrus only. The precentral gyrus of the frontal lobe (primary motor cortex) is commonly involved when the middle and anterior cerebral arteries are compromised. If the blood supply from the middle cerebral artery becomes affected, this will manifest as loss of sensation and motor function in the face and upper extremity while the compromise of the anterior cerebral artery will manifest as sensory and motor function loss in the lower extremity. The compromise of the middle and anterior cerebral artery can also be from surgery or manipulation of the carotid arteries. Surgeries on the common carotid arteries usually address severe stenosis from atherosclerosis. This procedure is called a carotid endarterectomy. With the carotid endarterectomy, there is a risk of creating a plaque embolism leading to occlusion of one of the cerebral arteries. Thrombosis formation after the procedure can also be possible. The thrombosis would lead to a unilateral decreased in the blood to the ipsilateral cerebral hemisphere. The feared complication of carotid endarterectomy is the rupture of the carotid artery leading to death.
Clinical Significance
The sensory homunculus can be useful in narrowing the area of infarction or ischemia in strokes. Even though most strokes involve the infarction or ischemia, both motor and sensory, the motor and sensory homunculus are so close together and have the same blood supply. This knowledge makes it possible to determine the artery that is most likely to be affected in strokes. The ischemia/infarction can be due to hemorrhagic bleeding, occlusion of the arteries, or merely a decrease in perfusion pressure.
If there is ischemia/infarction that affects the anterior cerebral artery, the individual will present with weakness, decreased, or complete loss of motor and sensory in the contralateral lower extremity. These findings are due to the perfusion territory of the anterior cerebral artery and the distribution of the homunculus.[12][13] While ischemia/infarction of the middle cerebral artery will manifest as defects in the contralateral upper extremity and the face. If both the middle and anterior cerebral arteries are affected, it will manifest as complete defects in the contralateral side of the body. If the individual were to have severe hypotension, the distal areas (watershed regions) of the perfusion territory of the middle and the anterior cerebral arteries would be affected, which will manifest as defects in the neck, shoulders, and torso, while the extremities and face are unaffected. These symptoms can also be present if the anterior and middle cerebral arteries' proximal blood supply is compromised. For example, if the internal carotid artery or common carotid artery has a decrease in perfusion pressure. The decreased perfusion pressure from the internal carotid artery and the common carotid artery can be due to occlusion from atherosclerosis, thrombosis, embolism, or external compression. But these etiologies of decreased blood supply through the carotid arteries will most likely after one artery and manifest signs/symptoms unilaterally.[14][15][16]
Other Issues
Since the sensory homunculus represents where the terminal sensory impulses of the body end up in the cortical cortex. If the cerebral cortex is to become compressed or compromised due to mass effect. The results of the mass effect will manifest in the body like loss of sensation and motor function. The loss of sensation is usually coupled with motor function loss due to the motor homunculus on the precentral gyrus being located cephalad to the postcentral gyrus. While, if only the postcentral gyrus is affected, this will manifest as a purely sensory loss. Mass-effect on the brain can come in many forms, such as neoplasms, cysts, infections, traumas, and hematomas.
(Click Image to Enlarge)
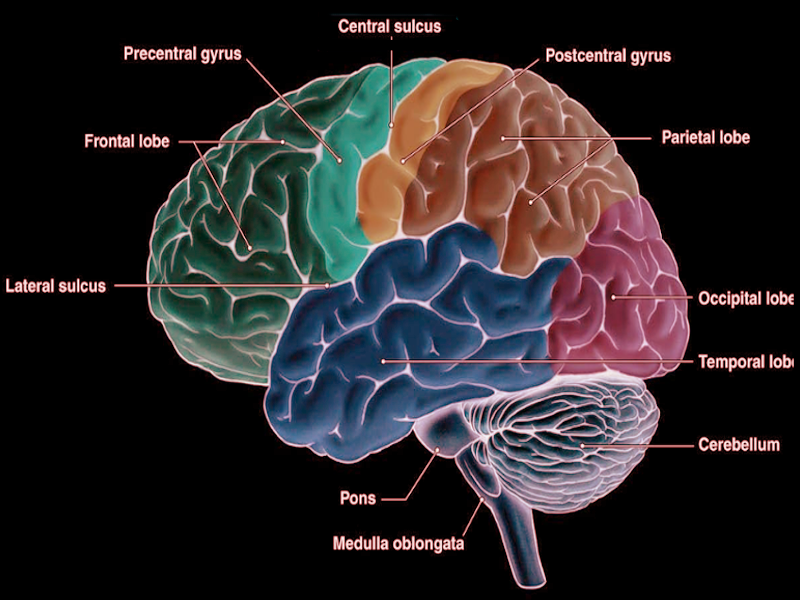
Precentral gyrus
Image courtesy Dr Chaigasame
(Click Image to Enlarge)
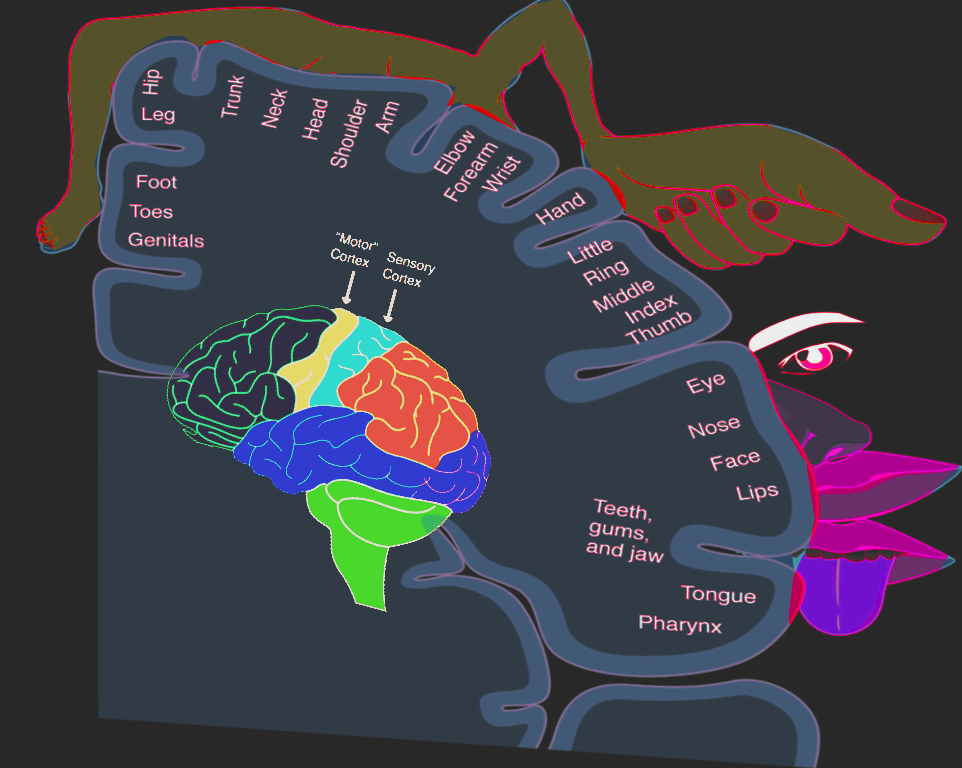
Homonculus: sensory & motor
Image courtesy S. Bhimji MD