Sternoclavicular Joint Injury
- Article Author:
- John Kiel
- Article Author:
- Subitchan Ponnarasu
- Article Editor:
- Kimberly Kaiser
- Updated:
- 9/7/2020 8:41:52 AM
- For CME on this topic:
- Sternoclavicular Joint Injury CME
- PubMed Link:
- Sternoclavicular Joint Injury
Introduction
Sternoclavicular (SC) joint injuries are uncommon.
The sternoclavicular joint is a diarthrodial joint composed of the sternum and clavicle. It is stabilized by the posterior capsular ligament which provides the most anterior-posterior stability and the anterior sternoclavicular ligament which restricts superior displacement. The costoclavicular ligament helps provide medial clavicle and anterior first rib stability. The interclavicular ligament passes over the sternum to provide medial traction of both clavicles. The inter-articular disc ligament attaches to the first rib and also provides stability of the sternoclavicular joint. In between the two articular surfaces and within the joint space is a fibrocartilaginous articular disc which functions as an important shock absorber. It is the only synovial articulation between the upper limb and axial skeleton. The subclavius muscle also supports the integrity of the joint. There are vital anatomic structures behind the clavicle which include the innominate artery and vein, vagus nerve, phrenic nerve, internal jugular vein, trachea, and esophagus. The medial clavicle physis appears in late adolescence and does not ossify until the age of 25.
Movement of the joint occurs from transmission of movement from the scapula and the rest of the shoulder girdle. In abduction, the sternoclavicular joint has 35 degrees of range. Anterior-posteriorly it can move 70 degrees. There is also a rotational component.
Injuries to the sternoclavicular joint can be traumatic or atraumatic. In traumatic injuries, the mechanism is usually a high energy injury such as a motor vehicle accident or injury during contact or collision sports. A sprain of the joint can occur when no laxity or instability occurs. Anterior dislocation is more common than posterior, which are associated with greater morbidity due to adjacent mediastinal and vascular structures. Atraumatic subluxations occur in younger patients with overhead elevation of the arm. This most commonly affects adolescent females with multidirectional instability. The subluxation is often painless and does not affect activities of daily living. It can be associated with trapezius palsy or spinal accessory nerve palsy.
Etiology
Spontaneous atraumatic subluxation of the sternoclavicular joint can occur. The typical patient is a female with multidirectional instability and ligamentous laxity. There is an excessive but incomplete translation or rotation of the medial clavicle away from the sternum. This is often referred to as a sprain.
Sternoclavicular dislocation refers to complete rupture of all the sternoclavicular and costoclavicular ligaments. This occurs from a single, well-defined trauma most commonly a motor vehicle accident or collision sport such as rugby or American football. The force is typically indirect on the shoulder. Most commonly, this is from an anterolateral or posterolateral force vector directed at the shoulder.
Epidemiology
Injuries to the sternoclavicular joint represent only 3% to 5% of all injuries to the shoulder girdle. Injuries at the acromioclavicular and glenohumeral articulations occur far more frequently. The most common cause is motor vehicle accidents followed by athletic injuries in contact and collision sports and then falls. For this reason, most patients are active young males.
Sprains of the joint and non-displaced medial clavicular physis fractures are more common than dislocations. In evaluating sternoclavicular joint disease, it is important to distinguish from a medial clavicle physeal fracture. The medial physis is the last growth plate to fuse in adults occurring around the age of 20-25.
Pathophysiology
A sternoclavicular joint injury is a rare injury to the shoulder girdle[1]. This is because the more peripherally placed bones and joints of the shoulder girdle tend to receive more of the energy from blunt trauma. The relatively strong, well reinforced sternoclavicular joint requires a substantial force of a specific vector to disrupt the joint space. Mechanisms significant to produce such a force include fall from height, contact and collision sports, and motor vehicle accidents.
Trauma may be directed at the medial clavicle or more commonly from an indirect blow to the shoulder. The mechanism typically determines the type of sternoclavicular dislocation. In anterior dislocations, the force is typically directed anterolaterally at the shoulder pushing the shoulder back and forcing the clavicle anteriorly on the medial side. Conversely, a posterolateral vector will push the shoulder anteriorly leading to a posterior clavicle dislocation. Although less common, a posterior clavicle dislocation can also occur from direct trauma to the medial clavicle.
Sternoclavicular subluxations can occur after anterior dislocations with the failed healing of ligamentous structures or spontaneously. Most commonly, this is seen in females with multidirectional instability. This can be associated with trapezius nerve palsy.
History and Physical
Patients with this injury will typically complain of anterior chest and shoulder pain often after significant trauma. This pain also can be insidious with no history of trauma. They will often localize their shoulder pain to the sternoclavicular joint. They may describe recurrent subluxation where the clavicle subluxes out with particular movements but reduces spontaneously when the arm is returned to neutral.
On exam, the clinician may appreciate prominence of the sternum or clavicle depending upon the degree of injury, mechanism, and whether there is an anterior or posterior dislocation. The affected shoulder will appear shorter. Abducting and elevating the arm should exaggerate the prominence. The subcutaneous location of the joint makes swelling an early exam finding. The patient may have pain, tenderness, edema, and ecchymosis over the affected joint space. The arm and shoulder will likely have decreased range of motion. Turning one’s head to the affected side may relieve the pain. The pain is often worse with movement or lying supine.
Anterior-posterior stability can be assessed by grasping the mid clavicle and applying translational force in the coronal plane. The amount of translation should be compared to the contralateral side. In grade I sprains, no instability should be appreciated. Grade II and grade III injuries can be more difficult to distinguish clinically. Grade III injuries typically have greater pain over the affected joint than grade II. Manually stressing the joint should demonstrate instability of the joint in grade II injuries; in grade III the swelling may be too great and or there may be a fixed dislocation.
In anterior dislocations, the patient is unlikely to have an injury to any other thoracic structures. Posterior dislocations are more serious and require a thorough assessment. The patient may have symptoms suggesting more significant mediastinal injuries such as dyspnea, stridor, dysphagia, or paresthesia. The clinician may observe tachypnea or hypoxia, respiratory distress, difficulty controlling secretions, discoloration, swelling, or decreased pulses of the affected limb.
Evaluation
Radiographs are the initial imaging modality of choice in suspected sternoclavicular separations or dislocations. Anterior-posterior views may be helpful; lateral views are unlikely to be of significant utility to assess the joint due to superimposed structures. The serendipity view, obtained by tilting the beam 40 degrees cranial can help better assess the sternoclavicular joint. A Hobbs view may also be obtained. In anterior dislocations, the affected clavicle will be visualized above the contralateral clavicle; in posterior dislocations, the opposite is true.
In suspected or radiograph-confirmed sternoclavicular dislocations, CT scan is the imaging study of choice. This provides a multiplanar evaluation of the joint space with three-dimensional reconstruction. In posterior dislocations, CT images can better visualize the mediastinal structures and co-occurring injuries. In children, it is also important to distinguish from a physeal fracture, which is better visualized on CT. Angiography should be utilized if the vascular injury is suspected.
Ultrasound can be used to identify posterior dislocations; however, it does not provide the same evaluation as CT scan when available. MRI may have some utility in evaluating ligamentous injury but should be ordered at the discretion of one’s consultants.
Treatment / Management
Atraumatic subluxations and chronic anterior dislocations can be managed nonoperatively with reassurance[2]. Generally, this includes a sling for comfort, which can be weaned, physical therapy, analgesia, and a graded return to play and activity. Grade I sprains can resolve in one to two weeks[3]. Grade II sprains can be managed conservatively as well; however, due to partial tearing of ligamentous structures, management requires a greater course of immobilization and protection. These patients may require a figure-of-eight brace as well.
Acute anterior dislocations of the sternoclavicular joint are controversial, primarily because it is a rare injury and difficult to study under controlled settings[4]. Because most anterior dislocations have a minimal long-term functional impact on quality of life, non-operative management is typically recommended, but the decision is made at the discretion of the orthopedic surgeon. Most surgeons recommend at least attempting closed reduction under general anesthesia, although residual instability of the joint space is commonpontaneous atraumatic anterior subluxation of the sternoclavicular joint[5]. In most cases, the risk of surgery outweighs the benefits.
Acute posterior dislocations less than 3 weeks old without evidence of mediastinal injury can be managed with closed reduction under general anesthesia. The standard technique is similar to anterior dislocations, where abduction and traction are used. If reduction is unstable or unsuccessful, the patient will have to decide whether to tolerate the deformity or an orthopedic surgeon can also perform an osteotomy of the medial clavicle.
Acute posterior dislocations with any evidence of vascular injuries, including decreased peripheral pulses, mediastinal injuries such as dysphagia, or pulmonary injuries such as shortness of breath need emergent open reduction and internal fixation with thoracic or vascular surgeons on stand-by[6]. It is also worth noting case reports of complications arising from unreduced posterior dislocations without any initial evidence of mediastinal injury. Thus, it can be argued that a failed closed reduction of posterior dislocation is an indication for open reduction and internal fixation.
Chronic or recurrent dislocations, anterior or posterior, as well as chronic pain at the sternoclavicular joint, are candidates for medical clavicle osteotomy.
Differential Diagnosis
The differential diagnosis of traumatic sternoclavicular injury is broad and includes fracture (sternum, clavicle, rib), sternoclavicular sprain, subluxation, or dislocation (anterior, posterior). Non-traumatic causes of sternoclavicular pain include arthropathies (osteoarthritis, rheumatoid, seronegative, crystal), infection (septic arthritis or osteomyelitis), SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis) syndrome, condensing osteitis, Friedrich disease, and multidirectional instability.
Staging
Sternoclavicular joint injuries are categorized as the following 3 stages:
- Stage I: Sprain (ligaments intact)
- Stage II: Subluxation (tearing of sternoclavicular ligaments; costoclavicular ligaments intact)
- Stage III: Dislocation (tearing of all ligaments)
Instability can further be described as follows:
- Degree: subluxation or dislocation
- Direction: anterior or posterior
- Etiology: traumatic or traumatic (congenital, developmental, spontaneous)
- Severity: sprain, subluxation, dislocation
- Duration: acute, chronic, recurrent, congenital
Prognosis
The prognosis for sternoclavicular injuries is generally favorable. In sprains or grade I injuries, the ligamentous structures are intact, and patients will make a full recovery in 1 to 2 weeks. In grade II injuries in which there was a traumatic or spontaneous subluxation, recovery takes longer. There is a possibility of cosmetic sequelae but typically not functional sequelae.
Anterior dislocations generally do well. Management is controversial and should be done in conjunction with an orthopedic surgeon. Because posterior dislocations have a high rate of complication, they are a surgical emergency requiring orthopedic consultation and reduction. If there is any evidence of injury to the neurovascular or mediastinal structures, open reduction and internal fixation are indicated emergently. However, most patients do well after treatment of the sternoclavicular joint injury.
Complications
The most common complications of a sternoclavicular joint injury are pain and cosmetic deformity of the joint. Patients are at risk of developing sternoclavicular arthritis, and that risk increases with the degree of injury. Complications of surgical management are significant and include hardware migration, infection, recurrence of dislocation, and non-cosmetic results.
Retrosternal or posterior dislocations can be associated with significant complications. Injury to the trachea, esophagus, brachial plexus and great vessels occur in 30% of posterior dislocations. There are several case reports of death from this injury. Specific injuries include esophageal or tracheal compression, pneumo- or hemothorax, tracheoesophageal fistula, ipsilateral acromioclavicular dislocation or clavicle fracture, compression of subclavian artery or vein, compression of the innominate artery, late subclavian vein obstruction, laceration of the innominate vein, or brachial plexus compression. These symptoms typically improve with surgical reduction of the sternoclavicular joint.
Postoperative and Rehabilitation Care
After closed reduction of acute anterior dislocations, the patient is immobilized in a sling. Depending on the stability of the joint, the patient is weaned out earlier (stable) or later (unstable) with progressive elbow and glenohumeral range of motion exercises. After closed reduction of acute posterior dislocations, the patient is immobilized in a figure-of-8 strap for at least 6 weeks. Active strengthening and range of motion exercises can begin around 12 weeks.
Consultations
Simple sternoclavicular joint sprains can be managed without consulting a sports medicine physician or orthopedic surgeon. If there is any concern about dislocation, the patient should be evaluated in the emergency department. Acute anterior dislocations may be a candidate for closed reduction at the discretion of the orthopedic surgeons. Posterior dislocations are a surgical emergency requiring consultation with an orthopedic surgeon, as well as a vascular and/or thoracic surgeon.
Deterrence and Patient Education
There are no clear guidelines for the prevention or deterrence of sternoclavicular joint injuries.
Patients should be aware that this is a rare cause of shoulder pain. Although spontaneous subluxations can occur, most are caused by high trauma such as a motor vehicle accident or collision in sports. Typically there is pain, swelling, and deformity at the joint. If the patient experiences these symptoms, they should be evaluated emergently. Most sternoclavicular joint injuries are managed nonoperatively. If they are dislocated posteriorly, an orthopedic surgeon is likely to surgically fix that dislocation due to the risk of secondary injuries.
Pearls and Other Issues
- Sternoclavicular injuries are rare due to the strong ligamentous support of the joint.
- A significant force is required to cause a dislocation although spontaneous subluxation can occur.
- If suspicion for sternoclavicular joint injury exists, the patient should be evaluated emergently.
- Although radiographs can be helpful, the diagnosis is made with CT.
- Most patients can be managed nonoperatively with analgesia, rest including a sling or figure-of-8 brace, physical therapy, and a graded return to activities of daily living.
- Reduction of acute anterior or posterior dislocations should be done in consultation with an orthopedic surgeon.
- Posterior sternoclavicular joint dislocations are a surgical emergency requiring evaluation by an orthopedic surgeon due to the proximity of the great vessels and mediastinal structures.
- In patients younger than 25, the provider also needs to consider medial clavicle physeal fracture.
Enhancing Healthcare Team Outcomes
The majority of patients with sternoclavicular injury present to the emergency room, the primary care provider or nurse practitioner. The majority of the mild injuries are managed without consulting a sports medicine physician or orthopedic surgeon. If there is any concern about dislocation, the patient should be evaluated in the emergency department. Acute anterior dislocations may be a candidate for closed reduction at the discretion of the orthopedic surgeons, but posterior dislocations are a surgical emergency requiring consultation with an orthopedic surgeon, as well as a vascular and/or thoracic surgeon at the time of surgical reduction.[7][8]
The outlook for most anterior dislocations are good but posterior dislocations have a guarded prognosis. Many patients with posterior dislocations also have other injuries and may have residual chronic pain or limited range of motion, despite treatment.[9][10] (Level V)
(Click Image to Enlarge)
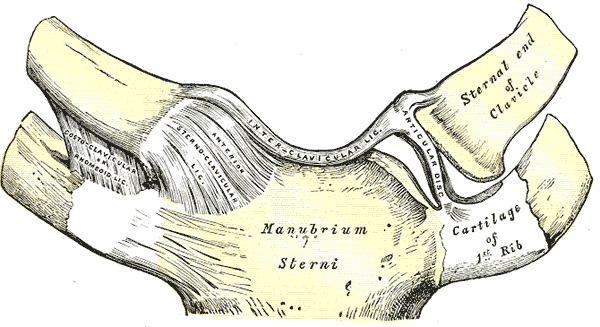
Sternoclavicular articulation, Anterior view, Manubrium, Sterni, Cartilage, First Rib, Ribs, Sternal end, Clavicle, Interclavicular Ligament, Anterior Sternoclavicular ligament, Costoclavicular, Anomeoid Ligament, Sternum
Contributed by Gray's Anatomy Plates