Anatomy, Shoulder and Upper Limb, Subscapularis Muscle
- Article Author:
- Kenneth Aguirre
- Article Author:
- Andrew Mudreac
- Article Editor:
- John Kiel
- Updated:
- 8/10/2020 5:18:55 PM
- For CME on this topic:
- Anatomy, Shoulder and Upper Limb, Subscapularis Muscle CME
- PubMed Link:
- Anatomy, Shoulder and Upper Limb, Subscapularis Muscle
Introduction
The subscapularis muscle is a large and powerful triangle-shaped muscle originating at subscapular fossa and inserting at the lesser tubercle of the humerus. The muscle derives its name from its orientation under the scapula: sub (under) scapula (wing bone). The subscapularis is one of the four muscles which compose the rotator cuff apparatus. The other three are the supraspinatus, infraspinatus, and teres minor muscles. The subscapularis muscle’s primary function is internal rotation, but can also aid in adducting the humerus. The subscapularis nerve innervates the muscle. The subscapular artery provides blood supply, and lymph drainage flows into the axillary nodes. This muscle and tendon are less likely to tear than other rotator cuff muscles. When there is an insult to the muscle or tendon, loss of function produces weakness in internal rotation. Non-operative management is the treatment of choice for partial tears and tendinopathies. Surgical intervention may be required (1) if conservative management fails, (2) depending on the activity level or profession of the individual, for example, athletes, and (3) in the case of full-thickness tears.[1][2][3]
Structure and Function
The subscapularis is the largest, strongest muscle of the rotator cuff. The rotator cuff muscles are important in shoulder movement and help maintain glenohumeral joint stability. The subscapularis muscle lies at the anterior surface of the scapula. It originates at the subscapular fossa, specifically the medial and lower two-thirds of the groove on the lateral border. The muscles transition to a tendon, which inserts on the lesser tubercle of the humerus in front of the joint capsule. Some fibers extend to the greater tubercle and bicipital groove. An outpouching of the glenohumeral joint lies between the subscapularis muscle and anterior surface of the scapula functioning as a bursa. The remainder of the rotator cuff muscles (supraspinatus, infraspinatus, and teres minor), insert into the greater tubercle. When the subscapularis muscle contracts, it will internally or medially rotate the humerus. The subscapularis is the only rotator cuff muscle that has this function. In certain positions, subscapularis has some adduction and extension functions. This function also helps prevent anterior displacement of the humerus.
Embryology
There are three primary germ layers, comprised of endoderm, ectoderm, and mesoderm during embryogenesis. The subscapularis muscle derives from mesoderm, as do all of the rotator cuff muscles.
Blood Supply and Lymphatics
The subscapular artery, a branch of the axillary artery, is the primary blood supply to the subscapularis muscle. Lymph drains into the axillary lymph nodes.
Nerves
The subscapular nerve originates from branches of the posterior cord of the brachial plexus (C5 to C7) and trifurcates into the upper, middle, and lower subscapular nerves. The upper and lower subscapular nerves innervate the subscapularis muscle. The upper subscapular nerve innervates the cranial half of the muscle, while the lower subscapular nerve bifurcates into two branches with the cranial branch innervating the caudal half of the muscle. The inferior branch of the lower subscapular nerve provides innervation to the teres major and the middle scapular nerve, also known as thoracodorsal nerve, innervates the latissimus dorsi muscle.
Muscles
The subscapularis muscle originates at the subscapular fossa and inserts into the lesser tubercle of the humerus. The muscle internally rotates and adducts the humerus. The bicep tendon lies underneath the subscapularis tendon in the bicipital groove.
Physiologic Variants
There are no known physiologic variants of the subscapularis muscle.
Surgical Considerations
Treatment for partial tears is non-operative. Surgical evaluation occurs when there is a full-thickness tear, depending on the activity level or profession of the individual, and patients who fail conservative management. Surgery is performed either by arthroscopy or open technique. Biceps pathology frequently co-occurs and may require tenotomy or tenodesis.[4][5][6][7]
Clinical Significance
Causes of shoulder pain due to subscapularis etiology may include tendonitis, tendinopathy, and tears. Tendonitis of the subscapularis is usually due when it comes in contact with the coracoid process from overuse in throwing or overhead athletes. Tendinopathy occurs when the symptoms become more chronic, and remodeling of the tendon begins to occur. Rotator cuff tears tend to occur with chronic degenerative tears from over-head use or acutely in athletes with overhead motion. The incidence of subscapularis tears is less than that of other rotator cuff tendons. When tears do occur, it is due to an anterior shoulder dislocation, fall on the outstretched arm during shoulder abduction, iatrogenic following anterior shoulder surgery, lesser tubercle avulsion, or associated with rotator cuff tear.[8]
History and Physical
Although any patient can injure their subscapularis tendon, they most commonly occur in young males. In acute injuries, the patient will likely report a history of forced external rotation. The patient will primarily complain of pain in front of the shoulder. A focused physical exam will include inspection, palpation, the range of motion, strength, and special tests. On physical exam, there may be weakness or pain with internal rotation weakness at 0 degrees and increase passive external rotation. The patient may be tender on the tendinous insertion of the upper arm along the lesser tubercle. The provider should perform a full examination of the shoulder as the patient may have injuries to other rotator cuff muscles or the biceps.
Multiple special tests can prove useful to examine the subscapularis. The "Gerber" or lift-off test is performed by having the patient internally rotate their shoulder and place the dorsum of their hand against their lower back. A positive test is when the patient is unable to move the hand away from the lower back with or without resistance or when they experience pain. If the patient is unable to get their hand behind their back, the abdominal compression or belly-press test may be employed. This test involves having the patient internally rotate their arm to their abdomen, with their elbow bent to 90 degrees, and the hand, wrist, and elbow forming a straight line and then pressing against the abdomen. A positive test is when the elbow falls posteriorly, with pain or weakness with the maneuver, or with the inability to compress without flexing the wrist. The bear hug test is performed by having the patient place their hand on the opposite shoulder. The examiner tries to externally rotate the arm while the patient tries to maintain their hand on the shoulder. A positive test occurs when the patient cannot hold against the external force applied by the examiner. The Napoleon test is performed similarly to the abdominal compression test. A positive result occurs when the patient can press only by flexing the wrist to 90 degrees and an intermediate result, suggesting partial function of the subscapularis muscle, occurs when the wrist flexes between 30 and 60 degrees.[9]
Imaging
Shoulder radiographs are typically first the first-line imaging modality for undifferentiated shoulder pain. In the case of a subscapularis injury, they are likely to be normal; however, an avulsion injury may produce a bony abnormality. In general, MRI is considered the best imaging modality to evaluate for rotator cuff injuries, including the subscapularis muscle. A tear of the subscapularis tendon can range from mild degenerative changes to a full-thickness tear of the tendon. The MRI can also evaluate the muscle belly as well. Diagnostic ultrasound is a cheap and easy modality to evaluate the subscapularis tendon in the hands of a skilled sonographer. Although it provides less detail than an MRI, it can help with diagnosis and management.[10]
Treatment
Subscapularis tendonitis and tendinopathy are managed conservatively. Generally, this includes rest and activity modification, including discontinuation of offending activities, analgesia including acetaminophen and NSAIDs, ice, and physical therapy. In most patients, this will resolve their symptoms. Refractory cases may indicate the need for corticosteroid injections.
Tears of the subscapularis tendon are often underdiagnosed and require a high index of suspicion by the clinician. Elderly patients with partial tear can be managed non-operatively with NSAIDs and physical therapy for 6 to 12 weeks. The short-term intra-articular injection can be effective for relieving pain and improving function. If no improvement with conservative management, then the patient should be referred to orthopedic for surgical evaluation. Athletes and younger individuals with a tear, as well as anyone with a full-thickness tear, should have a surgical evaluation. Surgery is performed either arthroscopically or in an open technique. Biceps pathology frequently co-occurs and may require tenotomy or tenodesis.
(Click Image to Enlarge)
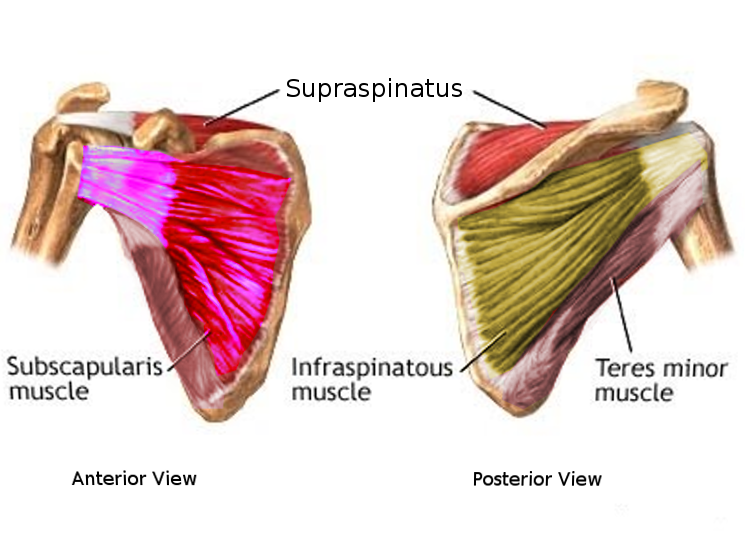
Subscapularis muscle
Image courtesy S Bhimji MD