Anatomy, Skin, Superficial Musculoaponeurotic System (SMAS) Fascia
- Article Author:
- Zackary Whitney
- Article Author:
- Megha Jain
- Article Editor:
- Patrick Zito
- Updated:
- 10/28/2020 1:02:19 AM
- For CME on this topic:
- Anatomy, Skin, Superficial Musculoaponeurotic System (SMAS) Fascia CME
- PubMed Link:
- Anatomy, Skin, Superficial Musculoaponeurotic System (SMAS) Fascia
Introduction
The superficial musculoaponeurotic system, or SMAS, is often described as an organized fibrous network composed of the platysma muscle, parotid fascia, and fibromuscular layer covering the cheek. This system divides the deep and superficial adipose tissue of the face and has region specific morphology. Anatomically, the SMAS lies inferior to the zygomatic arch and superior to the muscular belly of the platysma. The fibromuscular layer of the SMAS integrates with the superficial temporal fascia and frontalis muscle superiorly, and with the platysma muscle inferiorly. The SMAS is even often described as a fibrous degeneration of the platysma muscle itself. In reality, a precise anatomical definition of the SMAS is unclear and has been thoroughly debated since its first description by Mitz and Peyronie in 1976 [1].
Structure and Function
The SMAS connects the facial muscles to the dermis, and its purpose is to transmit, distribute, and amplify the activity of all facial muscles [2]. It has a close relationship with the most superficial fascial planes of the face and neck area. Macchi et al. describe the SMAS as a central tendon for a coordinated muscular contraction of the face and providing a functional role of movement for expression [3][4][3]
Embryology
The superficial facial musculature originates from the second arch mesenchyme which migrates during development and forms a pre-muscular lamina. This pre-muscular laminae ultimately gives rise to the mandibular, temporal, infraorbital, and cervical laminae during the eighth week of embryogenesis. The platysma muscle originates from a part of the cervical lamina which encloses the inferior portions of the parotid gland and cheek, while the SMAS derives from the superior portion [5].
Blood Supply and Lymphatics
The Superficial musculoaponeurotic system receives its blood supply from the Transverse facial artery, which also supplies blood to a broad region of the lateral malar area of the face. As this vessel courses directly through the SMAS, there is a risk of transection of this vessel during SMAS elevation. SMAS elevation is a step in facelift surgeries, technically known as "rhytidectomy" and also for facial reconstruction[6] following parotidectomy procedures. Therefore great caution is vital to evade any imminent danger to the transverse facial artery and even the neurovascular structures that lie close to this area.
The SMAS also partially receives arterial supply from the musculocutaneous perforators of the facial artery.
The small lymphatic vessels lying deep to the SMAS mainly flow into the preauricular or submandibular lymph nodes, which then drain into the anterior cervical chain.
Nerves
The branches of the Facial nerve are the most anatomically relevant nerves that lie in the vicinity to the SMAS and the facial muscles & associated fascial layers.
The facial nerve exits the skull inferior to the tragus of the ear. The proximal branches of the facial nerve primarily the temporal, zygomatic, and marginal mandibular nerves course deep to the SMAS after exiting the parotid gland.
Despite the anatomic disparity that exists, the superior masseteric retaining ligament and zygomatic ligament form a groove through which the Upper Zygomatic branch of the facial nerve traverses.
Another nerve worth listing is the Great auricular nerve. This nerve originates from the cervical plexus, passes inferiorly to traverse the sternocleidomastoid muscle about 6-cm inferior to the auditory canal, and runs just deep to the SMAS along the course of the external jugular vein.
The only nerves which traverse superficial to the SMAS are the sensory branches from the trigeminal nerve.
Muscles
The SMAS is considerably apparent in the buccal, temporal, zygomatic, and platysma regions. Thus, the corresponding muscles correlate or serve as an anatomical border to the SMAS.
The SMAS additionally invests smaller and more intricate muscles. This muscle group includes the orbicularis oculi, orbicularis oris, the occipitofrontalis, and the levator labii superioris muscle.
The forehead, nasolabial folds, and nasal regions are usually not included under the SMAS, although literature reporting several anatomical variants involving these muscles are available.
Physiologic Variants
There are several physiologic variants of the SMAS, but the bulk of differences seem to exist due to lack of uniform large-scale cadaveric studies employing histological and macroscopic dissection. The study by Khawaja et al. analysed the SMAS during 800 facelift procedures. They used the term SMAFS which stands for the superficial musculoaponeurotic fatty system instead of SMAS. From this research, they concluded that Six definite SMAFS variants exist. These six variants are - membranous, fatty, mixed (membrane-fatty, fleshy-fatty, among others), island (broken), fleshy, and fibrous. The variants described in this study are mainly due to the diversity in the deeper fatty layers of the SMAS. Some variants may be due to congenital anomaly or atrophy and breakage from repeated botox injections or even steroid use. They determined that the variants of SMAFS had an impact on the procedure and outcome of facelift surgery. The operative technique of plicating, lifting, debulking, and attaching the SMAFS to the bony periosteum has to be according to the type of SMAFS present, which is necessary for suitable cosmetic and surgical success.[4]
Surgical Considerations
The SMAS plays a vital role in the rhytidectomy, frequently known as the facelift procedure. Surgical manoeuvring and tightening of the SMAS allow for complete facial rejuvenation. The SMAS is more valuable to the enhancement of the lower third of the face than the midface. The clinical utility of the SMAS is primarily recognised in aesthetic surgery and employed in procedures to reverse age-related drooping of facial fat. These surgeries involve the superior elevation of the SMAS to elevate superficial dermal and muscular structures. Case reports suggest that 50% of all rhytidectomies consists of at least some type of SMAS manipulation and dissection. The studies hence portray the clinical and surgical significance of the SMAS in cosmetic and dermatologic surgical procedures[7][8][9][8].
Other Issues
As described previously, there have been numerous attempts to delineate and provide a more clear anatomical definition of the SMAS. However, inconsistencies exist not just regarding its anatomical location, but of its general morphology and basic terminology as well. There are even some researchers who doubt its existence. One of the main disagreements involves zygomaticus muscle investiture by the SMAS. Machi et al. reported through histological studies that the SMAS does indeed invest the zygomaticus muscle, while Gassner et al. argue that it does not. Another inconsistency often discussed is its continuity with the parotid fascia. Previous studies are somewhat inconclusive on this point.
In contrast, the majority of recent studies concur that the SMAS is an entirely separate layer that lies superficial to the fascia of the parotid gland or parotideomasseteric fascia. The anterior relationship to the nasolabial fold is also controversial. Still, most agree there is continuity with the nasolabial fold and even extension into at least some part of the orbicularis oris. Despite these discrepancies, the SMAS certainly plays a vital role in providing facial elasticity and support, while also facilitating coordination of muscular activity of the cheek.[10]
(Click Image to Enlarge)
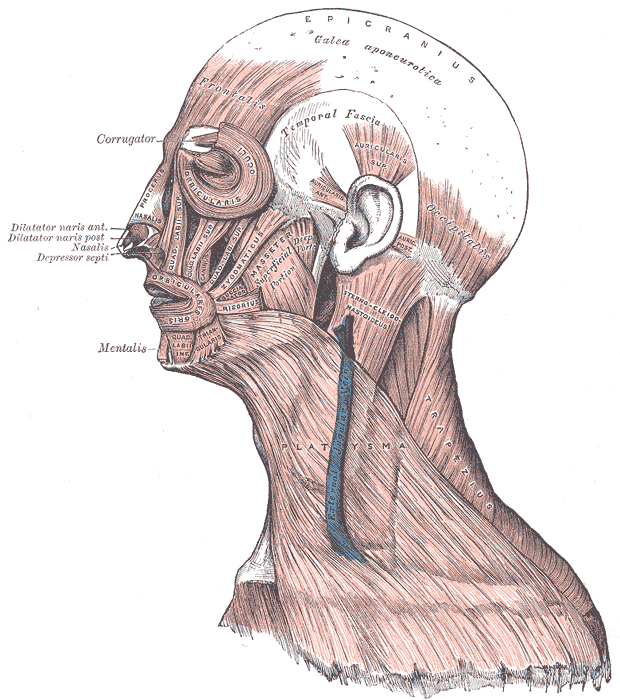
Head Face and Neck Muscles, Epicranius, Galea aponeurotica, Frontalis, Temporal Fascia, Auricularis Superior, Auricularis Anterior, Auricularis Posterior, Occipitalis, Sternocleidomastoid, Platysma, Trapezius, Orbicularis Oculi, Corrugator, Procerus Nasalis, Dilatator Naris Anterior, Dilatator Naris Posterior, Depressor Septi, Mentalis, Orbicularis Oris, Masseter, Zygomaticus, Risorius
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)

Frontalis Muscle: Anatomy of the forehead 1. Frontalis muscle 2. Brow fat pad 3. Orbital orbicularis oculi 4. Lateral orbital orbicularis (responsible for descent of the lateral brow) 5. Depressor supercilii 6. Corrugator supercilii 7. Supratrochlear nerve 8. Supraorbital nerve at supraorbital notch 9. Medial branch of the supraorbital nerve 10. Lateral branch of the supraorbital nerve 11. Temporal fusion line (temporal crest or linea temporalis) 12. Conjoint "tendon" 13. Frontal branch of the facial nerve
Contributed by Prof. Bhupendra C. K. Patel MD, FRCS