Anatomy, Bony Pelvis and Lower Limb, Superficial Peroneal (Fibular) Nerve
- Article Author:
- Alexandrea Garrett
- Article Editor:
- Zachary Geiger
- Updated:
- 8/10/2020 5:53:13 PM
- For CME on this topic:
- Anatomy, Bony Pelvis and Lower Limb, Superficial Peroneal (Fibular) Nerve CME
- PubMed Link:
- Anatomy, Bony Pelvis and Lower Limb, Superficial Peroneal (Fibular) Nerve
Introduction
The superficial peroneal nerve is also known as the superior fibular nerve. The superficial peroneal nerve originates from the common peroneal nerve alongside the deep peroneal nerve. The superficial peroneal nerve is the smaller of the two nerves.[1] The common peroneal nerve is comprised of fibers from spinal nerves L4 through S1 which itself originates from the bifurcation of the sciatic nerve which is composed of nerve fibers from spinal nerves L4 through S3. The sciatic nerve terminates and bifurcates at the apex of the popliteal fossa and becomes the common peroneal nerve and the tibial nerve as it wraps around the fibular neck.[2][3] After bifurcation from the common peroneal, the superficial peroneal nerve courses within the peroneus longus muscle.[1] This nerve thus provides motor innervation to the peroneus longus muscle. Additionally, the nerve also innervates the peroneus brevis muscle.[1] The nerve exits through the peroneal muscles on the anterolateral aspect of the lower half of the lower leg approximately 12 cm above the ankle joint at a defect in the crural fascia also known as the deep fascia of the leg.[1] The remainder of the nerve has sensory function provided by two branches inferiorly which are known as the medial dorsal cutaneous nerve (the larger of the two branches) and the intermediate dorsal cutaneous nerve. These nerves provide sensory innervation to the anterolateral aspect of the leg, the dorsum of the foot, and the dorsal aspect of the toes with the exception of the first web space.[1] The first web space is innervated by the dorsal peroneal nerve.[4]
Structure and Function
The superficial peroneal nerve has both motor and sensory components. The motor component of the nerve innervates the lateral compartment of the lower leg which includes the peroneus longus and peroneus brevis muscles. Motor activation of these muscles by the superficial peroneal nerve is primarily responsible for eversion and mild plantar flexion of the foot.[5] The peroneus longus muscle is also involved in maintaining support for the arch of the foot.[6][5]
The medial dorsal cutaneous nerve and intermediate dorsal cutaneous nerves are the terminal branches of the superficial peroneal nerve. These nerves handle the sensory component of the superficial peroneal nerve to the dorsum of the foot although it does not provide sensory innervation to the first webspace. Instead, the dorsal peroneal nerve provides sensory innervation to this area.[1][4]
Blood Supply and Lymphatics
The lateral compartment of the lower leg in which the superficial peroneal nerve lies receives its vascular supply predominantly from the fibular artery and the posterior tibial artery.[1] However, the superficial peroneal nerve itself receives blood supply from the anterior tibial artery as well as it courses towards the dorsum of the foot.[7][8][9] Because the nerve often runs alongside small perforating cutaneous arteries from the anterior tibial artery, including the superficial peroneal nerve accessory artery, skin flaps or segments of skin including this nerve, known as superficial peroneal neurocutaneous island flaps, have been used for skin grafting purposes and foot reconstruction.[7][8][9] However, the superficial peroneal nerve accessory artery has been shown to be absent in some patients.[8]
Muscles
The superficial peroneal nerve supplies motor innervation to the following muscles:
- Peroneus longus muscle
- Peroneus brevis muscle
Physiologic Variants
Anatomic variations of deep (crural) fascia piercings have been widely identified for the superficial peroneal nerve.[10][11][12] It appears that the superficial peroneal nerve pierces the crural fascia as a single nerve then bifurcates into the medial dorsal cutaneous nerve and intermediate dorsal cutaneous nerve as described above approximately 82.7% of the time known as the Type 1 variant.[10] However, approximately 15.6% of the time, it appears that the superficial peroneal nerve bifurcates early, therefore piercing the fascial layer as the medial dorsal cutaneous nerve and intermediate dorsal cutaneous nerve separately. This anomaly is known as the Type 2 variant.[10] Moreover, 1.8% of the time, there is documentation of a Type 3 variant in which the superficial peroneal nerve pierces the fascial layer as a single entity and continues as the normal course for the medial dorsal cutaneous nerve without evidence for an intermediate dorsal cutaneous nerve.[10]
In addition to variation in fascial layer piercings, the superficial peroneal nerve has also been shown to be located in various compartments of the leg rather than the normal lateral leg compartment. According to one study in India, 28.3% of cadaveric specimens were found to have the superficial peroneal nerve located in the anterior compartment.[11]
Surgical Considerations
The superficial peroneal nerve is the only nerve that can be visualized in the human body without dissection by simply plantar flexing, inverting the ankle, and examining the dorsum of the foot.[13][14][15]Despite its straightforward visualization, damage to the superficial peroneal nerve is the most commonly reported complication when performing ankle arthroscopy likely resulting from the fact that anterior ankle arthroscopy is typically performed in the neutral or slightly dorsiflexed position rather than the plantarflexed and inverted position.[14] Complication rates as high as approximately 17% have been reported, with more than 25% of those complications related to superficial peroneal nerve damage.[13] The recommendation is to visualize the nerve first and mark its course on the skin preoperatively to avoid damage.[14][16]
It is important to consider the anatomic variations of the superficial peroneal nerve and its branches as the branch most commonly at risk for iatrogenic injury is the intermediate dorsal cutaneous nerve when it courses near the distal fibula and both the medial and intermediate dorsal cutaneous nerves at the level of the ankle.[12]
Clinical Significance
When the superficial peroneal nerve is injured, one will lose the ability to evert the foot based upon the motor mechanics of the nerve.[1] The dorsum of the foot will exhibit loss of sensation (excepting the first webspace between the great toe and second toe where the deep fibular nerve provides sensory innervation).[1][4] The nerve damage pattern can accompany damage directly to the common peroneal nerve which frequently occurs due to a blow to the lateral side of the knee or a fracture to the fibular head.[1][3] The superficial peroneal nerve can also become trapped, and this can result in pain and paresthesias over the lower leg as well as the dorsum of the foot. Entrapment of the nerve can be secondary to an ankle sprain or twisting injury to the ankle which causes the nerve to stretch in the lower leg or foot.[17] Additionally, the nerve can also become entrapped by the fascia in a patient with either acute or chronic compartment syndrome resulting in reduced blow flow and oxygen delivery to the nerve. Surgical decompression is required to provide relief from pain and other symptoms especially in the acute setting.[18]
(Click Image to Enlarge)
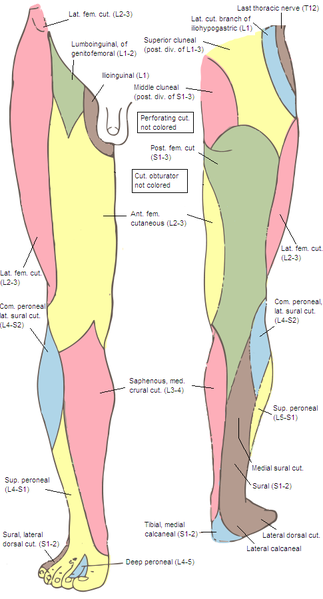
Lower limb, Peroneal Nerve
Contributed by Wikimedia Commons (Public Domain)
(Click Image to Enlarge)
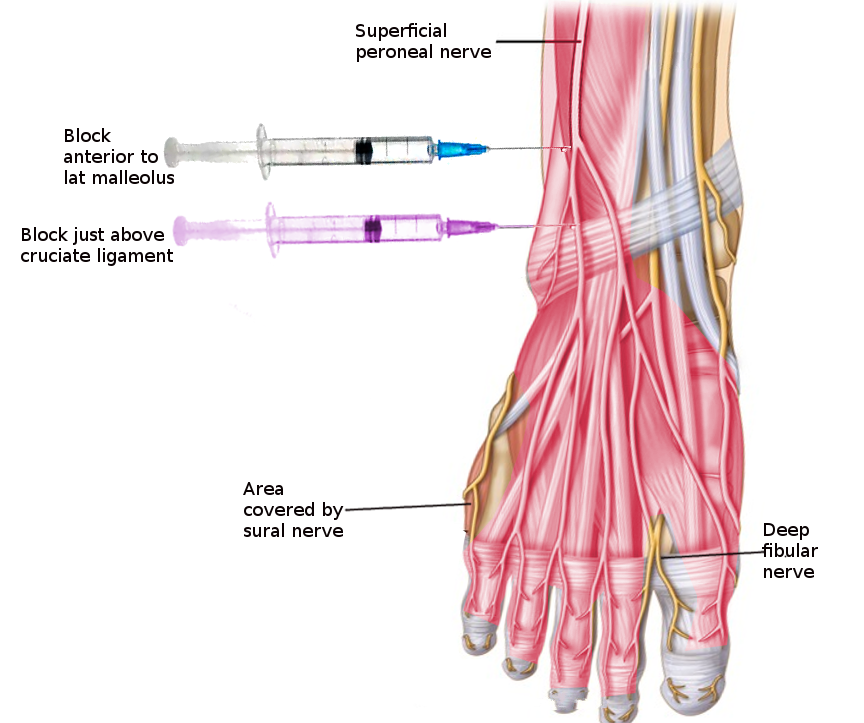
Superficial Peroneal Nerve block
Image courtesy S Bhimji MD