Neuroanatomy, Superior Petrosal Sinus
- Article Author:
- Matthew Koh
- Article Editor:
- SoHyun Boo
- Updated:
- 7/31/2020 3:17:46 PM
- For CME on this topic:
- Neuroanatomy, Superior Petrosal Sinus CME
- PubMed Link:
- Neuroanatomy, Superior Petrosal Sinus
Introduction
The superior petrosal sinus is a part of the dural venous sinus system that drains venous blood and cerebrospinal fluid circulating within the cranial cavity. The dural venous sinus system empties into the internal jugular vein and further flows into the cardiovascular circulation via the superior vena cava. Specifically, the superior petrosal sinus receives blood from the cavernous sinus and superior petrosal venous complex and drains into the transverse sinus. The superior petrosal sinuses are bilateral structures. These sinuses are between the middle and posterior cranial fossa. Because of their proximity to various critical intracranial structures, it is a significant landmark in surgical and interventional approaches to the skull.[1][2]
Structure and Function
Like the other portions of the dural venous sinus system, the composition of the walls of the superior petrosal sinus is dura mater lined with epithelium. These walls lack valves and vessel layers. The course of the superior petrosal sinus is as follows: the sinus originates in the cavernous sinus, leaves the posterosuperior aspect of the cavernous sinus, then runs caudally between CN III and IV. The sinus then joins with the transverse sinus. The skull contains the superior petrosal sulcus—a groove in the temporal bone—through which the superior petrosal sinus runs. The tentorium cerebelli is attached to the edges of the superior petrosal sinus.[2][3]
The function of the superior petrosal sinus is to pass blood from the cerebral veins and cerebrospinal fluid from the subarachnoid granulations into the transverse sinus. After traveling through the rest of the dural venous sinus system, this venous fluid will drain via the internal jugular vein. The fluid then empties into the superior vena cava and the systemic circulation.[1][2]
Embryology
The dural venous sinuses develop accordingly with the meningeal layers of the brain, specifically the dura mater. The superior petrosal sinus develops last in the major sinuses and is derived from the mesencephalic vein, a pro-otic vein, during the development of the cerebellum.[4]
The superior petrosal sinus attains its position in the adult brain by the physical expansion of the growing temporal lobe during development. Early in development, the superior petrosal sinus, oculomotor nerve, and trochlear nerve are close to the anterior dural fold and well in front of the otic capsule. As the temporal lobe grows, it presses the anterior tentorial layer backward, pushing the superior petrosal sinus towards the otic capsule. Thus, the cranial nerves and the superior petrosal sinus attain their adult positions along the border of the otic capsule.[3]
Blood Supply and Lymphatics
Other than the cavernous sinus, the superior petrosal sinus receives vascular supply by the superior petrosal venous complex (SPVC). The SPVC is one of the largest veins in the posterior fossa. The tributaries of the SPVC include the veins of the cerebellopontine fissure, veins of the middle cerebellar peduncle, and the transverse pontine and pontotrigeminal veins.[1][2][5]
Physiologic Variants
The superior petrosal venous complex drains into the superior petrosal sinus; there are three different identified drainage pattern variants. Type I describes a superior petrosal venous complex that empties into the superior petrosal sinus above and lateral to the boundaries of the internal acoustic meatus. Type II describes drainage between the lateral trigeminal nerve and the medial facial nerve at the internal acoustic meatus. Type III describes drainage above or medial to the Meckel cave. Of the three types, Type II is the most common drainage pattern.[5]
Surgical Considerations
Because the tentorium cerebelli is attached to the edges of the superior petrosal sinus, during surgical procedures, the superior petrosal sinus is useful as a landmark. The tentorium cerebelli is also used to classify the location of tumors. Herniation of the brain through the tentorium cerebelli may require surgical intervention.[6]
The drainage pattern of the superior petrosal venous complex into the superior petrosal sinus can determine the surgical approach in neurosurgical procedures. For example, surgeons use the retrosigmoid suprameatal neurosurgical approach in type II and III cases. To better outcomes, before surgery, CT angiogram and magnetic resonance venogram can be used to visualize the junction of the superior petrosal venous complex and the superior petrosal sinus to determine the drainage pattern. The correct classification of superior petrosal venous complex drainage pattern and imaging can guide both the surgical approach and division of the superior petrosal sinus and the tentorium cerebelli.[5][7]
Clinical Significance
The superior petrosal sinus is especially clinically relevant when involved in conditions such as carotid-cavernous fistulas and dural arteriovenous fistula malformations (AVFMs). AVFMs are abnormal connections between meningeal arteries and dural sinuses. Arteriovenous fistula malformations can classify into three categories: Type I, II, and III. To clarify, this classification system differs from the method used to classify the drainage pattern of the superior petrosal venous complex into the superior petrosal sinus. Type I AVFMs drain directly into meningeal veins or dural venous sinuses. Type II AVFMs are Type I AVFMs, but additionally, this type has retrograde drainage into subarachnoid veins due to high pressure. In contrast, Type III AVFMs do not have meningeal or dural venous sinus drainage and drain solely into subarachnoid granulations.[8]
Arteriovenous fistula malformations involving the superior petrosal sinus are definitively treatable with either surgery or endovascular therapy.[9] Of the endovascular therapies, transvenous embolization is the nonsurgical treatment of choice for Type I, II, and III AVFMs; transarterial embolization can also be performed but may be more challenging to achieve definitive treatment.[8] If preservation of venous flow is necessary, transarterial embolization or surgery are both options. Furthermore, transvenous embolization can be used preoperatively to minimize bleeding and complications. Endovascular embolization allows for closure of the AVFM or effective preoperative treatment.[9]
Another therapy for superior petrosal sinus AVFM is gamma knife radiosurgery. However, gamma knife-induced closure of the fistula requires up to three years. As a result, gamma knife radiosurgery is not a viable therapy in high-grade AVFMs but may be an option in low-grade AVFMs. Unfortunately, superior petrosal sinus AVFMs are typically high-grade.[9] Additionally, the proximity of the superior petrosal sinus to the brainstem can result in radiation-induced deleterious effects.[2][10]
(Click Image to Enlarge)
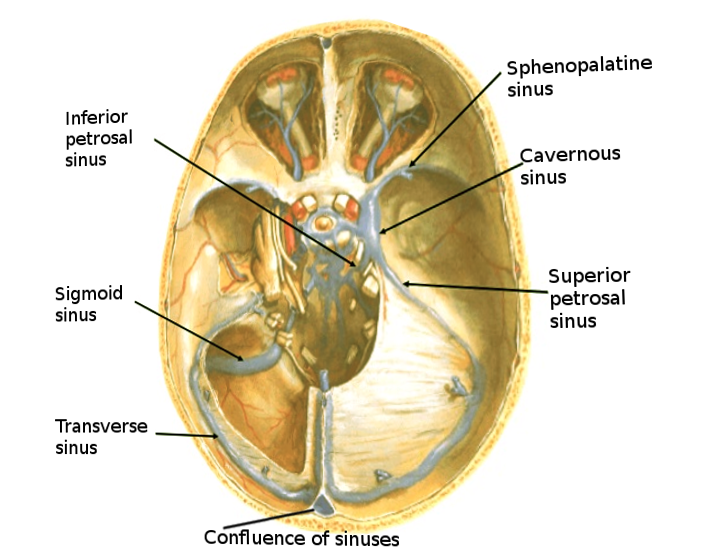
Brain sinuses
Image courtesy S Bhimji MD
(Click Image to Enlarge)
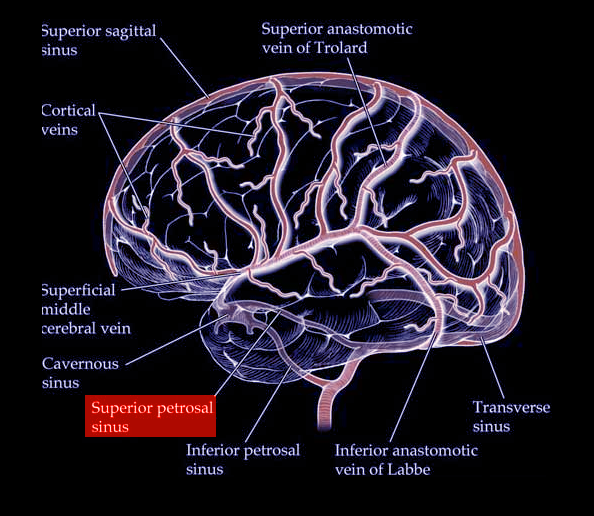
Brain sinuses
Image courtesy S Bhimji MD