Physiology, Taste
- Article Author:
- Fahad Shaikh
- Article Editor:
- Abhinandan Soni
- Updated:
- 4/29/2020 2:56:44 PM
- For CME on this topic:
- Physiology, Taste CME
- PubMed Link:
- Physiology, Taste
Introduction
The human body has certain types of general sensations, e.g., touch, pressure, etc. and certain special sensations such as smell and sight. One of these special sensations is taste. Technically known as gustation, this sense serves to provide the ability for one to discern the characteristics of substances that one ingests. At a basic evolutionary level, taste allows one to assess whether these substances are nutritious or potentially hazardous. This sensation is primarily relayed via receptors located on the tongue, but at the higher cortical level, taste is considered a multisensory experience since the smell of a particular food item, its texture, and whether or not it activates pain receptors (e.g., spicy food) all play a role in determining how it “tastes.”[1] This article aims to review the pertinent anatomical, neurological, and molecular factors associated with the physiology of taste, and discuss its clinical relevance.
Cellular
Taste is sensed by chemosensory receptors known as taste buds. Taste buds themselves consist of columnar cells arranged circumferentially to form a single “taste pore” between them, and microvilli extending from the columnar cells arranged around this pore. These microvilli are the location of the actual taste receptors, which are coupled to ion channels in the apical membrane and are responsible for sensing taste stimulus. Nerve fibers are associated with the basolateral surface of these cells and are responsible for conducting impulses to the central nervous system.
Development
The primary organ associated with taste reception is the tongue, and understanding taste reception and the relevant anatomy requires knowledge of the tongue’s anatomy.[2] The tongue itself divides into two separate regions, derived from different embryological structures, and a third area also comes into play when discussing taste and its innervation. The anterior two-thirds of the tongue, the area in front of the terminal sulcus, arises from the 1 and 2 pharyngeal arches, and as such derives its innervation from the Mandibular division of the trigeminal nerve for somatosensation (touch, pain, pressure, etc.), and the chorda tympani branch of the facial nerve for taste sensation. The posterior third of the tongue, behind the terminal sulcus, arises from the third pharyngeal arch and derives both taste and somatosensation from the Glossopharyngeal nerve. The third part refers to the upper esophageal area, and the vagus nerve innervates the root of the tongue, which also expresses taste receptors.
The tongue contains three types of papillae, the circumvallate, along the terminal sulcus, fungiform, on the anterior surface of the tongue, and foliate papillae on the lateral surface of the tongue.[3] Taste buds distribution is relative to these papillae; they also appear on the palate, tonsillar pillars, epiglottis, and upper esophagus.
Organ Systems Involved
Taste reception and conveyance involve the tongue to send primary taste input, but the olfactory system also plays an essential role in how tastes are perceived. Taste is not a standalone sensation; how one perceives taste is inexorably linked with the smell of the stimulus as well.[4] This fact is evident when one has a cold or other nasal obstruction, and tastes seem blunted. The peripheral and central nervous systems are also involved with taste sensation, as they are with all other sensations, as pathways relay taste sensation from receptor organs to the central nervous system.
Function
Taste is functionally crucial for a few reasons. Taste sensation can change according to the body’s specific nutritional needs at different points in time, thereby guiding an organism to particular sources of whatever nutrient it needs, eg. Salt depleted animals in which adrenalectomy has been performed will choose drinking water that has a higher content of salt to replete body stores.[5] As mentioned earlier, specific fundamental characteristics of taste such as bitterness may denote substances that are harmful or poisonous for the body, and thus would make one consciously aware, and may prevent one from ingesting them.
Once taste signals reach the central nervous system, multiple reflex pathways are activated that lead to the body “preparing” for a meal, with increased salivation, and elevated secretory activity in the stomach.[6] The above examples make it clear that taste has a vital role to play in normal physiology.
Mechanism
The mechanism of taste signals converting from the form of a chemical stimulus to electrical impulses for transmission to the brain requires the use of specific ion channels and second messenger systems. The type of system utilized for transduction depends upon the taste itself.[7] The different forms of tastes recognized include salty, acidic, sweet, bitter, and umami (described as a “meaty” taste derived from amino acids in food, especially glutamate). The form of transduction used for bitter as well as sweet tastes is G-protein coupled receptors, while acidic and salty foods lead to direct activation of ion channels that cause nerve signal propagation. Umami taste sensation appears to involve both G-protein coupled receptors as well as ion channels.
As molecules of food enter the oral cavity, they reach “taste pores” on the apical surface of taste buds surrounded by microvilli known as “taste hairs,” binding to specific receptors on the cell surface and result in depolarization or activation of intracellular signaling by second messengers, depending on the type of taste sensation.[8] There may be an influx of calcium ions, causing vesicles to exocytose their neurotransmitter contents, results in the formation of an action potential and subsequent signal transduction along the basolateral surface of the taste receptors, which then transmits as electrical impulses along nerve fibers.
Following the creation of electrical impulses, they potentiate along their nerve pathways.[9] For example, fibers carrying taste sensation from the anterior two-thirds of the tongue move along the lingual nerve to the chorda tympani branch, which joins the facial nerve as it courses through the middle ear cavity, or via the glossopharyngeal or vagus nerves depending from where the taste signals originate. All these signals travel to a single brainstem nucleus, the nucleus of the tractus solitarius. From there, these impulses continue to the ventral posteromedial (VPM) nucleus of the thalamus, and then relayed by third-order neurons to higher-level cortical taste centers (which include part of the insular cortex) and these signals are then consciously appreciated. Some information is also conducted to the hypothalamus, where the lateral and dorsomedial nuclei play an important role in regulating eating behaviors. These nuclei are affected mainly by the hormones leptin and ghrelin, which mediate the balance between satiety and hunger.
Related Testing
"Taste" testing involves assessment of gustatory and olfactory function, and in some rare cases, imaging or electrogustometry is necessary.[10] Gustatory testing can involve the use of spatial tests, taste sticks, tasting tablets, and olfactory testing commonly involves the use of the UPSIT (University of Pennsylvania Smell Identification Test). Imaging may be useful if there is a concern for some sort of mass lesion affecting the taste pathway, and bacterial culture may be done if there is clinical suspicion of infection leading to taste dysfunction.
Pathophysiology
Taste may be affected in many clinical conditions due to inflammation and damage of specific neural pathways involved in taste sensation; this may be due to infection, drugs, radiation, etc. Chemical stimulus appreciation may be affected by mineral deficiencies, e.g., zinc. Impairment of smell due to any reason can also have negative impacts on taste perception, as mentioned above.
Clinical Significance
Taste may be affected in many clinical conditions, such as upper respiratory and middle ear infections, since the facial nerve passes through the middle ear along its course to the central nervous system. Bell palsy can often present with taste disturbance as well. Radiation therapy is also a common etiology of taste disturbances, designated post-irradiation gustatory dysfunction.[11] Taste loss is associated with a decrease in appetite and food intake, and especially in patients who have undergone radiotherapy for malignancy; this can increase the risk of cancer cachexia and severe weight loss, and have a negative impact on overall prognosis.[12] Adenoid hypertrophy in children links with olfactory disturbance, which can cause a lack of taste appreciation.[13] Nutritional deficiency of zinc has demonstrated to cause taste loss, with studies finding that deficiency of zinc due to any etiology was associated with varying degrees of taste abnormalities, and that zinc supplementation usually produced improvement in these abnormalities.[14] Taste may also be affected as a side effect of a multitude of drugs[15]; the antifungals griseofulvin and terbinafine, the antihypertensive angiotensin-converting enzyme (ACE) inhibitors, calcium channel blockers, and so on. The antibiotic Metronidazole is also associated with a metallic taste disturbance. Clinicians need to be aware of these side effects when prescribing medications, so they can convey accurate information to their patients and provide better care. Taste has a logical connection to overeating and obesity.[16] Obesity, being linked to diabetes, cardiovascular disease, and other causes of morbidity and mortality, has quickly become a global health concern, with about 39 % of the world's population considered to be overweight or clinically obese in 2018, a number that has undoubtedly grown exponentially.[17] Studies have found that abnormalities in the central response to taste can develop in individuals who suffer from obesity, and can be responsible for developing unhealthy eating patterns that can lead to exacerbation of obesity and difficulty in losing weight, as well as maintaining weight loss in previously obese individuals.[18] Carbohydrates especially have been shown to have a positive association with overeating. Taste has been an often ignored sensory modality, considered not to be as crucial as other senses, and patients may often decline to disclose whether they have taste disorders spontaneously. The question "Do you have a taste problem?" was only able to identify 10% of patients with taste problems. It is essential to directly approach this topic with patients and ask specific closed-ended questions to ensure appropriate history taking.[19] Taste loss may arise as a consequence of a diverse spectrum of systemic or acute clinical conditions or medications, and may well play a role in dealing with the worrisome obesity crisis that faces the world. From a hedonistic aspect, taste disturbance can also reduce the pleasure of life, and cause a significant reduction in patients' quality of life. It is important, therefore, to understand the anatomy and physiology associated with this basic sense.
(Click Image to Enlarge)
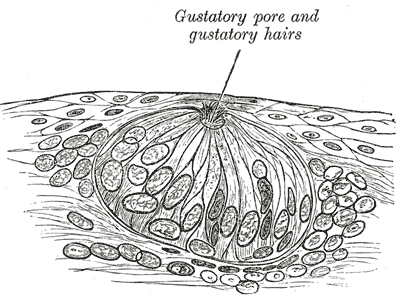
The Organs of the Senses and the Common Integumentary, Highly Magnified Tastebud
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)
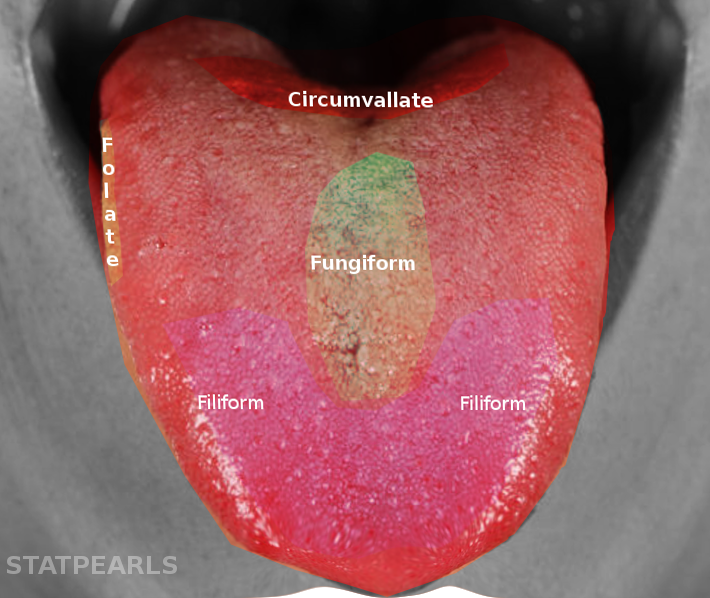
Tongue taste buds
Image courtesy S Bhimji MD
(Click Image to Enlarge)
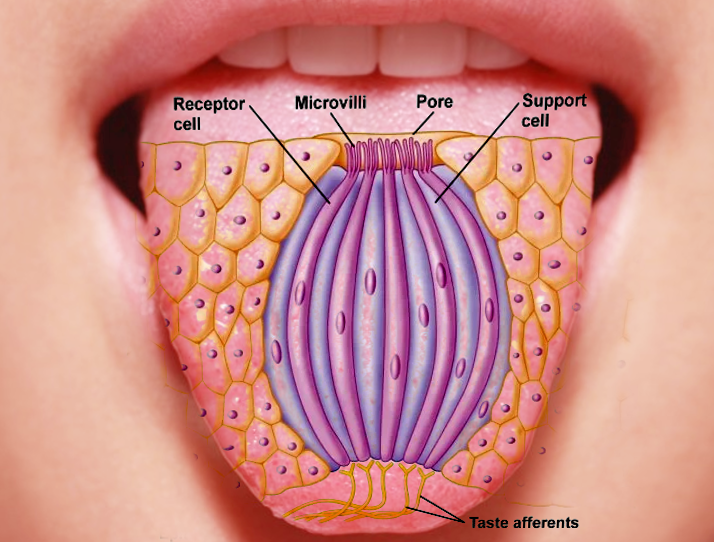
Taste bud histology
Image courtesy S Bhimji MD