Anatomy, Shoulder and Upper Limb, Arm Teres Minor Muscle
- Article Author:
- Pallavi Juneja
- Article Editor:
- John Hubbard
- Updated:
- 8/22/2020 8:56:48 PM
- For CME on this topic:
- Anatomy, Shoulder and Upper Limb, Arm Teres Minor Muscle CME
- PubMed Link:
- Anatomy, Shoulder and Upper Limb, Arm Teres Minor Muscle
Introduction
The teres minor is a narrow, intrinsic shoulder muscle that extends from the lateral border of the scapula to the greater tubercle (or tuberosity) of the humerus. It contributes to the “rotator cuff,” a capsule of muscles and tendons that collectively stabilize the glenohumeral joint. The teres minor is responsible for lateral, or external, rotation of the arm at the shoulder.[1][2][3]
Structure and Function
Anatomy
The teres minor arises from the posterior surface of the scapula, directly adjacent to the upper part of its lateral border. The upper fibers of the muscle culminate in a tendon that inserts on the greater tubercle of the humerus. The tendon blends into the capsule of the shoulder joint. The lower fibers of the muscle insert directly into the humerus, just below the greater tubercle.
The teres minor lies inferior to the infraspinatus and superior to the teres major; all three muscles have a similar oblique orientation. In anatomical position, the long head of the triceps brachii muscle is oriented perpendicular to the teres minor and inferior to it. The teres minor is deep to the deltoid muscle.
Function
As a rotator cuff muscle, the teres minor stabilizes the ball-and-socket glenohumeral joint by helping hold the humeral head (ball) into the shallow glenoid cavity of the scapula (socket). The teres minor also laterally, or externally, rotate the arm at the shoulder joint. As a lateral rotator, the teres minor is an antagonist muscle to medial rotation; therefore, the teres minor is especially critical in stabilizing the shoulder during medial rotation to prevent anterior dislocation of the humerus.
Embryology
The teres minor, a muscle of the upper limb, arises from the myotome of paraxial mesoderm (somites). The upper limb bud appears at about four weeks and lies opposite somites C4, C5, C6, C7, C8, T1, and T2. During week 5, the myotomes migrate into the limb bud and form 2 condensations: 1 posterior and 1 anterior. The posterior condensation gives rise to all intrinsic shoulder muscles, including the teres minor. The muscle groups are well-established by 8 weeks.
Blood Supply and Lymphatics
The teres minor is supplied by the subscapular artery and one of its branches, the circumflex scapular artery, as well as the posterior circumflex humeral artery. The subscapular artery and the posterior circumflex humeral artery arise from the third, most distal portion of the axillary artery.
The subscapular artery is the largest branch off of the axillary artery. It travels caudally before dividing into 2 arteries: the circumflex scapular and the thoracodorsal. The circumflex scapular artery travels around the lateral border of the scapula between the subscapularis and teres minor. It moves cranially through the triangular space, created by the teres minor superiorly, teres major inferiorly, and long head of the triceps brachii laterally, into the infraspinatus fossa where it joins the scapular anastomosis. Along its route, the circumflex scapular artery supplies the teres minor.
The posterior humeral circumflex artery is a more distal branch off of the third portion of the axillary artery. It travels posteriorly with the axillary nerve through the quadrangular space, bounded by the teres minor superiorly, teres major inferiorly, the surgical neck of humerus laterally, and long head of triceps brachii medially. Then the artery moves anteriorly around the surgical neck of the humerus to supply the shoulder joint. Along its route, the posterior humeral circumflex artery supplies the teres minor.
Nerves
The axillary nerve innervates the teres minor. The axillary nerve, composed of nerve roots C5 and C6, arises from the posterior cord of the brachial plexus. First, the axillary nerve is posterior to the axillary artery and anterior to the subscapularis muscle, then it travels to the inferior edge of the subscapularis muscle. Here, it moves posteriorly out of the axilla with the posterior circumflex humeral artery (PCHA) through the quadrangular space, created by the teres minor superiorly, teres major inferiorly, the surgical neck of humerus laterally, and long head of triceps brachii medially. When it enters the posterior scapula, the axillary nerve bifurcates into two terminal branches; the posterior terminal branch innervates the teres minor.
Muscles
The rotator cuff comprises 4 muscles: supraspinatus, infraspinatus, teres minor, and subscapularis. The supraspinatus, infraspinatus, and teres minor all arise from the posterior scapula and insert on the greater tubercle of the humerus. The subscapularis arises from the subscapular fossa of the anterior scapula and inserts on the lesser tubercle of the humerus.
Collectively, the rotator cuff stabilizes the glenohumeral joint, which is a far more shallow and unstable ball-and-socket joint than the hip. Each muscle also helps with certain movements of the arm. The supraspinatus is responsible for the first 15 degrees of abduction; the deltoid, an intrinsic muscle of the shoulder that is not a rotator cuff muscle, is responsible for abduction from 15 to 90 degrees. The infraspinatus and teres minor both aid in lateral, or external, rotation of the arm at the shoulder. The subscapularis, along with the teres major, another intrinsic muscle that is not part of the rotator cuff, and extrinsic muscles like the pectoralis major and latissimus dorsi, is responsible for medial, or internal, rotation of the arm.
Surgical Considerations
A rotator cuff tear, including a tear to the teres minor, will not heal without surgery; however, good function of the affected shoulder can often be gained non-surgically. Therefore, surgery is indicated if nonsurgical treatment fails and the patient experiences persistent pain or weakness, or if optimal function of the arm is required for overhead work or sports.[4][5][6][7]
The type of surgical repair depends on the type of tear. A "partial thickness" tear, or incomplete tear, may only require debridement, or removal of damaged tissue. A "full thickness" tear extends fully through the tendon, though it may only involve part of the tendon; it can be repaired using side-to-side sutures. The most common rotator cuff injury results in the tendon being pulled from its bony insertion termed a complete tear; this requires the tendon to be repaired directly back to the bone. Surgical repair can be open, with a large incision providing direct access to the injury, or arthroscopic, with 2 small incisions for passage of a camera (arthroscope) and tools for repairing any damage.
Clinical Significance
Assessment: Hornblower’s sign
Hornblower’s sign can be used to assess the teres minor for injury, particularly a tear. The patient’s arm should be placed to 90 degrees in the scapular plane with the elbow flexed to 90 degrees. The patient will then externally rotate against resistance, trying to make a “field goal” sign. The test is positive if the patient cannot externally rotate the shoulder, indicating teres minor pathology.[8][9][10]
Quadrangular Space Syndrome
Quadrangular space syndrome produces excessive or chronic compression on structures that pass through the quadrangular space, including the axillary nerve and posterior humeral circumflex artery. The syndrome can be caused by overuse of the arm, particularly in overhead activity, or traumatic injury, like a shoulder dislocation. The teres minor is innervated by the axillary nerve and supplied, in part, by the posterior humeral circumflex artery. Therefore, quadrangular space syndrome can result in selective atrophy of the teres minor, vague shoulder pain, and paresthesia.
Tendinitis
The rotator cuff muscle tendons, including the teres minor tendon, can be inflamed or irritated in a process called tendinitis. In general, tendinitis is usually an exertional injury caused by repetitive use; rotator cuff tendinitis is caused by repetitive use of the arm, often in overhead activities. The patient will present with pain or clicking when raising the arm above the head. Treatment is conservative, including rest, ice, and anti-inflammatory medications. Stretching and strengthening exercises help to reduce the load through the tendon. Cortisone injections can be used for refractory pain.
Shoulder Impingement Syndrome
Shoulder impingement syndrome is defined as compression or impingement of the rotator cuff tendons, including the teres minor, by the overhanging bone of the scapula called the acromion. Impingement is caused by narrowing of the space between the acromion and the rotator cuff, often due to repeated, overhead activity of the arm that inflames the rotator cuff tendons. Patients can present with shoulder pain, particularly when trying to lift an arm overhead or in conjunction with shoulder weakness. Treatment is conservative, including rest, ice, and anti-inflammatory medications. Physical therapy can help to rebuild strength and range of motion in the shoulder.
Tear
Any of the rotator cuff muscles, including the teres minor, can tear. Tears can either be acute or chronic. An acute tear usually results from falling on an outstretched arm or an attempt to lift something heavy. A chronic tear occurs over time and is usually secondary to tendinitis or shoulder impingement syndrome wearing away at the muscle. A rotator cuff tear will not heal without surgery; however, good function of the affected shoulder can often be gained non-surgically.
(Click Image to Enlarge)
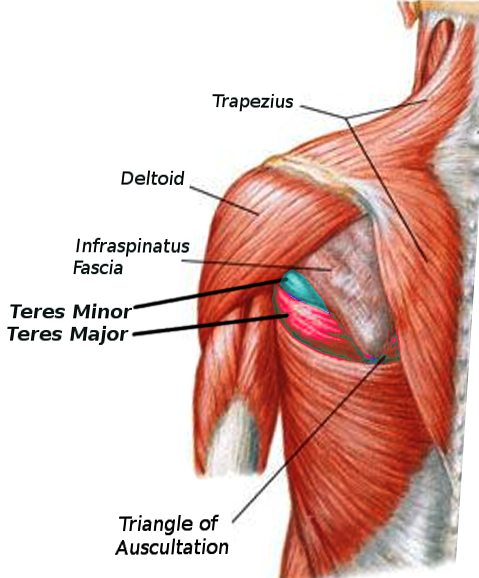
Teres Major and Minor
Image courtesy S Bhimji MD