Papillary Thyroid Carcinoma
- Article Author:
- Faten Limaiem
- Article Author:
- Anis Rehman
- Article Editor:
- Thomas Mazzoni
- Updated:
- 10/16/2020 6:17:02 PM
- For CME on this topic:
- Papillary Thyroid Carcinoma CME
- PubMed Link:
- Papillary Thyroid Carcinoma
Introduction
Papillary thyroid carcinoma (PTC) is an epithelial malignancy showing evidence of follicular cell differentiation and a set of distinctive nuclear features. It is the most frequent thyroid neoplasm and carries the best overall prognosis. The tumor usually appears as an irregular solid mass but in rare cases, it may have cystic features. One key feature of PTC is its ability to invade adjacent structures like lymphatics. About 10% of patients may present with metastatic disease at initial presentation. The overall prognosis is good for patients less than 45 years of age
Etiology
Known risk factors for PTC include:
Radiation exposure:The incidence of papillary thyroid cancer is greater in people who have a history of exposure to significant ionizing radiation.
Childhood exposure:External low-dose radiation therapy to the head and neck during childhood, used in the 1940s to 1960s to treat various benign diseases, predispose to PTC. The average time from irradiation to the recognition of the tumor is approximately 10 years but may be longer than 30 years.[1] Medical Therapy:High radiation doses (> 2000 cGy) used in the treatment of malignant diseases have also been associated with an increased risk of PTC. Environmental exposure:The Chernobyl nuclear accident, which occurred on April 26, 1986, led to a 3- to 75-fold increase in the incidence of PTC in fallout regions, especially in younger children.
Genetics:
There are few familial syndromes associated with PTC, including familial adenomatous polyposis—Gardner syndrome, Werner syndrome, and Carney complex type 1. Familial PTC cases have been reported in 5% of all patients with PTC and may portend a more aggressive disease course.[2]
There is also a higher incidence of PTC in regions with high dietary iodine intake and in patients who have preexisting benign thyroid disease.
Epidemiology
Papillary thyroid carcinoma is the predominant form of thyroid cancer accounting for 80-85% of all thyroid cancer cases In a report based upon the Surveillance, Epidemiology, and End Results (SEER) database from 1975 to 2012, the incidence of PTC increased from 4.8 to 14.9 per 100,000.[3][4] Papillary thyroid carcinoma occurs predominantly in middle-aged adults with a 3:1 female-to-male ratio and the median age at presentation is 50 years. Even though rare in children, PTC is still the most common pediatric thyroid malignancy. It affects whites more commonly than blacks.[5]
Pathophysiology
Chromosomal rearrangements have been identified in PTC and include the RET protooncogene, NTRK1, and the MET gene overexpression. Further, mutations in the BRAF gene have also been identified. A clear association between PTC and radiation exposure is now well established.
Histopathology
Gross findings:
Grossly, PTC typically presents as an invasive neoplasm with poorly defined margins, a firm consistency, and a granular white cut surface. Calcifications may be present. The size is widely variable, with a mean diameter of 2-3 cm. Papillary thyroid carcinoma has three classification categories based on the size and extent of the primary lesion. Minimal carcinoma or occult carcinoma/micro-carcinoma tumors are 1.5 cm or smaller and show no evidence of invasiveness through the thyroid capsule or to cervical lymph nodes. These lesions are typically nonpalpable and are usually incidental findings during operative or autopsy examination. Intra-thyroid tumors are greater than 1.5 cm in diameter but remain confined to the thyroid gland with no evidence of extra-thyroid invasion. Extra-thyroid tumors extend through the thyroid capsule to involve the surrounding viscera.[6]
Microscopic findings:
The two cardinal morphological features of conventional PTC are the papillae and nuclear changes. The papillae are composed of a central fibrovascular stalk covered by a neoplastic epithelial lining. The papillae may be long, straight, or arborizing; arranged in a parallel, regimented fashion; short and stubby, or tightly packed. The thickness and composition of the papillary stalk are variable. The stalk is usually made up of loose connective tissue and variously sized thin-walled vessels.[7]
The diagnosis of papillary carcinoma has as its basis the nuclear morphology of a thyroid neoplasm. The existence of multiple architectural variants proves the irrelevance of architecture. The following constellation of features characterize the diagnostic nuclear morphology [7]:
- Enlarged and elongated nuclei with crowding and overlap
- Irregular nuclear contour
- Chromatin clearing with peripheral margination of chromatin, giving rise to what has been described as Orphan Annie Eye nuclei
- Multiple micro-nucleoli located immediately underneath the nuclear membrane
- Nuclear grooves resulting from an irregularity of nuclear contour seen in 2 dimensions
- Intranuclear cytoplasmic pseudo-inclusions from the accumulation of cytoplasm in prominent nuclear grooves
- Another key feature of PTC is the presence of psammoma bodies
Immunohistochemical Findings:
Immunohistochemistry is seldom of value in diagnosing PTC although it may play a role in metastatic disease. The neoplastic cells are strongly and diffusely immunoreactive with keratin, CK7, thyroglobulin, TTF1, and PAX8, while other markers (HBME-1, Galectin-3, S100 protein, CITED1, CK19) yield variable results.[8]
History and Physical
Papillary thyroid carcinoma usually presents as an asymptomatic (painless) thyroid mass with or without enlargement of regional (cervical) lymph nodes. Hoarseness and dysphagia occur in approximately 20% of cases, signaling recurrent laryngeal nerve involvement with vocal cord paralysis or tracheal compression. Nodal metastases in the lateral neck are reported in 27% of patients at presentation most often originating from tumors in the ipsilateral thyroid lobe.[9]
The examination usually reveals a painless hard lesion that is usually less than 5 cm. The mass is usually fixed and has irregular borders.
Evaluation
Fine needle aspiration:
It is often is the initial diagnostic method used in the detection of PTC. Fine-needle aspiration specimens from conventional PTC are usually cellular and may show papillary structures, monolayer sheets, and 3D groups in a background of watery or thick so-called ropy colloid, nuclear or calcific debris, macrophages, and stromal fragments. The individual tumor cells are enlarged, elongated, or oval, with eosinophilic cytoplasm. The nuclei show elongation, membrane thickening, chromatin clearing, grooves, and pseudo-inclusions. These tumors usually show enlarged follicular cells arranged in monolayer sheets and follicular groups in a background of thin and thick colloid.[10][11]
Laboratory tests:
Thyroid function testing has limited utility in the diagnosis of PTC because most patients have normal thyroid function.[12]
Radiographic features:
On thyroid scan, PTCs typically appear as cold (hypo-functioning) nodules, but rarely can appear as hot (hyperfunctioning) nodules.
Ultrasound examination is the imaging modality of choice for PTC. Sonographic features include a hypoechoic or isoechoic solid nodule with irregular or poorly defined margins, micro-calcifications, taller-than-wide shape, and disorganized internal vascularity. Ultrasound findings are also invaluable for guiding fine-needle aspiration biopsy of abnormal nodes. Microcalcifications are highly specific for this cancer.
Other imaging modalities, including CT, MRI, and FDG-PET/CT, may be needed to assess the extent of extra-thyroidal extension, to evaluate the presence of substernal masses, to detect recurrent tumors, and to improve diagnostic accuracy.[13]
Treatment / Management
Surgery:
Primary treatment decisions have as their basis a preoperative risk assessment that includes clinical, imaging, and cytological data. Choices depend on the location and extent of identifiable disease and the risk that unidentifiable disease foci are also present. With increasing emphasis on risk-stratified management, the treatment approaches recommended by the 2015 ATA guidelines are more conservative than in the past.[14] A lobectomy is an option for unifocal tumors smaller than 4 cm with no evidence of extra-thyroidal extension or lymph node metastasis. For patients with PTC >4 cm, or with gross extra-thyroidal extension (clinical T4), or clinically apparent metastatic disease to nodes (clinical N1) or distant sites (clinical M1), the initial surgical procedure should include a near-total or total thyroidectomy and gross removal of all primary tumor unless there are contraindications to this procedure. If surgery is chosen for patients with thyroid cancer <1 cm without extra-thyroidal extension and cN0, the initial surgical procedure should be a thyroid lobectomy unless there are clear indications to remove the contralateral lobe. Thyroid lobectomy alone is sufficient treatment for small, unifocal, intrathyroidal carcinomas in the absence of prior head and neck radiation, familial thyroid carcinoma, or clinically detectable cervical nodal metastases.[14] Prophylactic central-compartment neck dissection (ipsilateral or bilateral) should be a consideration in patients with PTC with clinically uninvolved central neck lymph nodes (cN0) who have advanced primary tumors (T3 or T4) or clinically involved lateral neck nodes (cN1b), or if the information will be used to plan further steps in therapy.
Adjuvant Radioiodine Therapy:
After thyroidectomy, radioiodine is the therapy of choice in patients with PTC to ablate residual normal thyroid tissue.
Radioiodine therapy is indicated in the following cases [15]:
- Patients with tumor >2 cm and one of the following risk factors: gross extra-thyroidal extension, age >45 years, lymph node and distant metastases
- Patients with tumor <2 cm and distant metastasis
Radioactive iodine therapy is given 4-6 weeks after surgery. Prior to treatment, a hypothyroid state is induced by stopping thyroid hormone replacement treatment. The therapy is continued until no more radioactive iodine uptake is seen. Potential adverse effects of radioactive iodine include:
- Sialoadenitis
- Transient thyrotoxicosis
- Pulmonary fibrosis
- Emesis
- Brain edema (can be prevented with the use of corticosteroids)
- Infertility
- Small risk of leukemia, breast or bladder cancer
Thyroid Hormone Treatment:
After thyroidectomy, patients require lifelong thyroid hormone therapy, usually as monotherapy with levothyroxine (LT4). Since TSH can promote the growth of remaining PTC cells, the dosage of LT4 should initially be high enough to achieve suppression of thyrotropin. The thyroid function should be checked after 6 to 8 weeks. Depending on the result, the dosage should be adjusted; the use of TSH suppressive therapy should merit careful consideration since it carries an increased risk of complications.[14]
NCCN Guidelines for Total thyroidectomy:
- Known distant metastases
- History of radiation
- Extrathyroidal extension
- Bilateral nodules
- The tumor measures more than 4 cm
- Poorly differentiate lesion
- Positive cervical lymph nodes
Routine cervical node dissection continues to be debated. Some literature notes fewer recurrences but other studies note a higher incidence of recurrent nerve injury.
Differential Diagnosis
The primary differential diagnoses of PTC are:
- Reactive changes following fine-needle aspiration.[16] This condition characteristically shows nuclear enlargement, chromatin clearing, and micro-nucleoli similar to nuclei of PTC.
- Severe chronic lymphocytic thyroiditis, where the reactive atypia attributed to inflammation results in nuclear morphology similar to that of PTC.[17]
- Other differential diagnoses include adenomatoid nodules, diffuse hyperplasia, dyshormonogenetic goiter, follicular adenoma, follicular thyroid carcinoma, medullary thyroid carcinoma, and metastatic tumors.
Staging
Several staging systems have been proposed for PTC and continue to evolve. The most commonly used are [18][19][18]:
For patients less than 45 years:
- Stage l: any Tm any N, MO (cancer localized to the thyroid)
- Stage ll: Any T, any N, MI (cancer spread to cervical nodes or to distant organs)
For patients older than 45 years:
- Stage l: T1, N0, M0 (cancer less than 2 cm)
- Stage ll: T2, N0, M0, and T3 (cancer localized to the thyroid and is between 2-4 cm)
- Stage lll: T4, N0, MO, and any T, N1, M0 (lesion more than 4 cm and spread limited to the neck)
- Stage lV: Any T, any N, M1 (cancer spread outside the neck and to distant organs)
Prognosis
Although PTC frequently metastasizes to regional lymph nodes, it still generally carries an excellent prognosis. There are, however, several clinicopathological and background features that can lead to a poor prognosis.[20]
Poor prognostic factors of PTC include:
- Older age at diagnosis
- Large tumor size
- Extra-thyroidal growth
- Male sex
- Less differentiated or solid areas, vascular invasion, and aneuploid cell population
- Subtypes of PTC that associate with a more aggressive clinical behavior: tall cell variant, diffuse sclerosis variant, solid variant, and follicular variant
Complications
Extra-thyroidal extension:
Extra-thyroidal extension occurs in 8% to 32% of cases.[21]
Local or regional recurrences:
Local or regional recurrences occur in 5 to 15% of patients with PTC.[22]
Distant metastases:
Distant metastasis occurs in only 1% to 25% mostly in the lungs and bones. Other less common sites are the brain, liver, and skin.[23]
Postoperative and Rehabilitation Care
Long term monitoring is necessary every 6-12 months to look for recurrence for at least 5 years
Levels of TSH and thyroglobulin must be measured
Enhancing Healthcare Team Outcomes
Papillary thyroid cancer is ideally managed by an interprofessional team that consists of an endocrinologist, general surgeon, oncologist, radiation oncologist, nuclear medicine physician, internist, pharmacists, and specialty care nurses. The majority of patients present to the primary provider or nurse practitioner with a painless mass in the neck. Once the FNA is performed, the patient should be referred to an oncologist and a surgeon. Patients need to know that the sole treatment for PTC is surgery. Patients treated with radioactive iodine need to be educated about this therapy and warned about the potential adverse effects. Following surgery, the patient requires long term monitoring for recurrence. Most patients require long term thyroid hormone replacement. Specialty care nurses in oncology assist with treatment, monitor and educate patients, and provide updates to the team. [Level 5]
With early diagnosis and prompt treatment, the prognosis for most patients is excellent.
(Click Image to Enlarge)
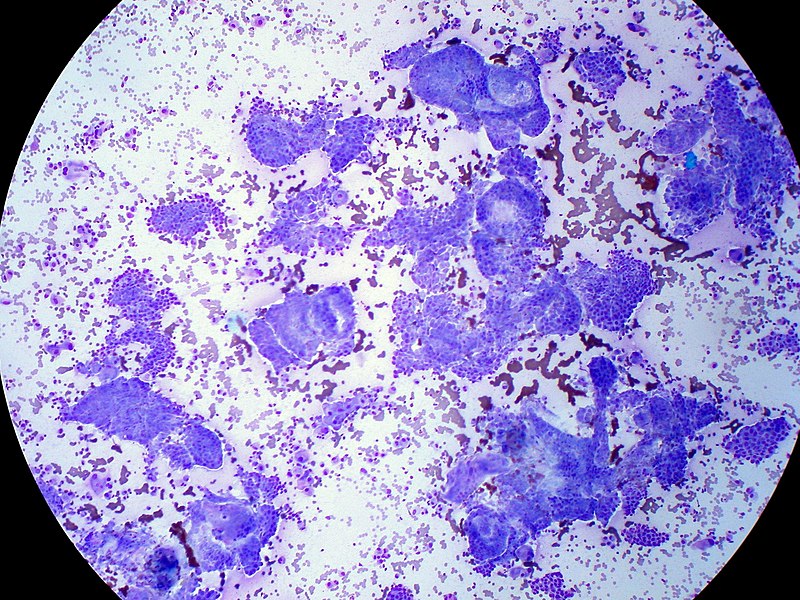
Papillary thyroid carcinoma , FNA giemsa stain
Conributed by Wikimedia User: Ed Uthman Source: https://commons.wikimedia.org/wiki/File:Papillary_Thyroid_Carcinoma,_FNA,_Giemsa_Stain_(7782080838).jpg (CC BY 2.0 https://creativecommons.org/licenses/by/2.0/deed.en)