Ethylene Glycol Toxicity
- Article Author:
- Aruba Iqbal
- Article Author:
- Jason Glagola
- Article Editor:
- Thomas Nappe
- Updated:
- 8/14/2020 9:16:49 PM
- For CME on this topic:
- Ethylene Glycol Toxicity CME
- PubMed Link:
- Ethylene Glycol Toxicity
Introduction
Ethylene glycol (C2H6O2) is a toxic alcohol that is found in various household and industrial agents. The term “toxic alcohols” is a collective term that includes methanol, ethylene glycol, and isopropyl alcohol. Ethylene glycol exposure can be extremely dangerous, with significant morbidity and mortality if left untreated. Ethylene glycol is a colorless, sweet-tasting liquid most commonly found in antifreeze, but occasionally used for other purposes, such as industrial solvents. Exposures are generally observed due to accidental or intentional ingestions, with its sweet taste lending to accidental toxic exposures, whereas intentional exposures may be motivated by suicide attempt or desire for inebriation in the absence of ethanol. Ethylene glycol exposures can cause varying degrees of toxicity and management generally requires supportive care, close laboratory monitoring and antidotal therapy. The primary treatments are either ethanol or fomepizole and, occasionally, dialysis. [1]
Etiology
Ethylene glycol toxicity is most commonly due to ingestion. It has fairly limited dermal absorption, unlike other alcohols, such as methanol.[2] Most exposures are intentional as sucide attempts or, occasionally, for inebriation. Children who may ingest antifreeze while exploring their enviornments may be prone to consuming significantly toxic amounts due to its sweet taste.[3]
Epidemiology
Individuals at risk include toddlers and young children exploring their environment, alcoholics, and suicidal individuals.[1] According to the Annual Report of the American Association of Poison Control Centers' National Poison Data System, the number of case mentions of ethylene glycol in 2016 was 6,374. The majority of these cases were in adults greater than 20 years old and were intentional[4]. Children under the age of 12 made up 686 of the known total 6,374 cases with 13 unknown child age cases[4].
Pathophysiology
Ethylene glycol is rapidly absorbed through the gastrointestinal tract after ingestion with serum concentrations peaking very soon after ingestion. The volume of distribution is about 0.7 L.kg. Elimination is primarily first order when concentrations are under 250 mg/dL, with a half-life of approximately 4-6 hours.[5] With concentrations above 250 mg/dL, elimination becomes zero order at likely around 10 mg/kg/hr. When alcohol dehydrogenase is inhibited, preventing metabolism, elimination half-life of ethylene glycol is prolonged to 10-18 hours and is renally dependent.[6][7]
Like ethanol and methanol, metabolism begins with gastric mucosal alcohol dehydrogenase, and occurs primarily in the liver through serial oxidation by alcohol dehydrogenase and aldehyde dehydrogenase, with each step reducing NAD+ to NADH. Ethylene glycol is first oxidized by alcohol dehydrogenase to glycoaldehyde, which is then oxidized by aldehyde dehydrogenase to glycolic acid, which is primarily responsible for the associated metabolic acidosis. Glycolic acid is then oxidized to glyoxylic by glycolic acid oxidase, or lactate dehydrogenase due to its resemblence of lactate. Glyoxylic acid is a precursor for oxalic acid, the nephrotoxic metabolite; and also for the nontoxic metabolites, α-hydroxy-β-ketoadipic acid and glycine, which is further converted to hippuric acid. Thiamine is a cofactor in the production of α-hydroxy-β-ketoadipic acid and pyridoxine and magnesium are cofactors in the production of glycine [1][8][9][10]
Toxicokinetics
A potentially lethal dose of ethylene glycol is approximately 1-2 mL/kg of 95% concentrated solution, or about 1,500 mg/kg.[11] Ethylene glycol, the parent compound, is inebriating but generally considered nontoxic. The parent compound is osmotically active, and is responsible for the increased osmolality observed in the early course of exposure prior to metabolism. Ethylene glycol's metabolites are responsible for the anion gap metabolic acidosis. Although there is evidence that each of the metabolites are toxic, it is glycolic acid that is believed to be long-lived enough to be primarily responsible for the anion gap metabolic acidosis, while oxalic acid is responsible for the associated end-organ injury, nephrotoxicity. Oxalic acid deposits in renal tubules as insoluble calcium oxylate monohydrate, leading to proximal tubular necrosis. Oxalic acid's affinity for calcium may lead to hypocalcemia, which can be associated with tetany, seizures, and QT interval prolongation on electrocardiogram. It is important to realize that the increased osmolar gap can be present early after toxic exposure prior to significant metabolism, but as the course progresses the osmolar gap closes, with metabolism leading to the development of an anion gap metabolic acidosis without increased osmolar gap.[11][8][9]
History and Physical
History is often challenging to acquire in an intentional, self-harm attempt or substance abuse scenario and physical exam can often be normal early in the course. Many patients may be embarrassed or may not want to admit to their actions. It is also common for patients to underestimate the magnitude and severity of their ingestion. Accidental ingestions, however, are often self-reported or witnessed. Many times, there is a diagnostic dilemma, and it is up to the clinician to consider toxic alcohol exposure as an etiology for a finding such as a metabolic acidosis with an elevated anion gap, or in this case, potentially with renal injury.[1]
Severity of illness will vary with time from exposure to presentation, if coingestion of ethanol has occurred, or if early treatment was accessible. Ethylene glycol toxicity usually presents with a varying degree of inebriation early in the course, with the potential for central nervous system depression (CNS). During this time, there is often an elevated osmolar gap without an elevated anion gap or acidosis. As the concentration of ethylene glycol shifts toward production of metabolites, the osmolar gap decreases and the anion gap increases with the development of a metabolic acidosis. Ingestion of ethanol at any point will halt the metabolism of ethylene glycol. As ethylene glycol is progressively metabolized over the course of 4-12 hours, an anion gap metabolic acidosis develops secondary to the accumulaiton of glycolic acid. During this time, the patient may feel generally ill or be CNS depressed, and may begin to compensate with hyperventilation or hyperpnea. Tachycardia and hypertension may also occur. After about 12 hours, there may be evidence of nephrotoxicity, demonstrated by elevated creatinine, due to the precipitation of calcium oxalate crystals in the proximal tubules. This caclium oxalate deposition may predisopose to hypocalcemia, placing patient at risk for tetany, seizures, QT interval prolongation and dysrhythmias. After about 12-18 hours, oliguira may develop. If treatment occurs during this time, the acute renal injury is normally reversible and dialysis is often unnecessary. However, if treatment is delayed further, usually by delayed presentation or recognition, acute renal failure and systemic illness may develop, including acute respiratory distress syndrome, cerebral edema or infarction, and heart failure. Multisystem organ dysfunction is believed to be associated with calcioum oxalate deposition. If treatment does not occur early enough, the course of illness can lead to coma and death. [12][11][13][8][9][10]
Evaluation
A patient who has ingested ethylene glycol will present somewhere along the spectrum of asymptomatic with an increased osmolar gap to very ill with end-organ toxicity and anion gap metabolic acidosis. The evaluation of the ethylene glycol intoxicated patient should follow a diagnostic approach that utilizes historical and objective data. An electrocardiogram, basic metabolic panel, and acetaminophen concentration should be obtained on all toxicology patients with suspected self-harm attempt. Additional tests to be considered when self-harm is a concern are a complete blood count, transaminases, lipase, pregnancy status, serum or urine ketones, lactate, ethanol and salicylate concentrations. In the case of toxic alcohols, salicylate toxicity is very important to rule out, especially when evaluating a patient with metabolic acidosis. Ethanol concentration is also required in the evaluation of a patient with toxic alcohol ingestion because ethanol inhibits the metabolism of ethylene glycol.[10]
Toxic alcohol concentrations are confirmatory and are measured by gas chromatography, which is not readily available in all healthcare facilities. Concentration is reported in milligrams per deciliter (mg/dL) and, since it typically peaks soon after absorption, is expected to decrease by zero-order kinetics as described above. The time of ingestion is also important to consider, as the toxic alcohol concentration may not reflect the level of toxicity if metabolism has already progressed. This is because it is the metabolites that are primarily responsible for the toxic effects. In the case of ethylene glycol, an oxalic acid concentration may be assessed to correlate with end-organ toxicity resulting in nephropathy; however, its upstream precursor, glycolic acid is the primary contributor toward acidosis.
Obtaining toxic alcohol concentrations often requires sending a serum sample to an outside facility, which may take hours to days to result, and diagnosis is usually required sooner. Therefore, a methodological approach to the diagnosis needs to be considered in which the patient is monitored for the anticipated effects of toxicity. Since anion gap acidosis is a later finding, a patient presenting with normal acid-base status early after ingestion should be observed for a minimum of 12 hours with serial basic metabolic panels every 2 to 4 hours to monitor for the development of metabolic acidosis and an elevated anion gap. This observation period can only begin once it is confirmed that the patient’s ethanol concentration is undetectable. It is also important to refrain from administering exogenous bicarobonate or prophylactic fomepizole during this observation period. A 12-hour observation period has been accepted as the standard of care, but it is based on collective experience more than specific data since acidosis is likely to occur earlier than 12 hours.[1]
Many prefer to utilize the measurement of the osmolar gap for further risk stratification in the early-presenting patient. An increased osmolar gap is nonspecific and indicates the presence of any osmotically active agent, such as an ethanol. There is an inverse relationship between the osmolar gap and the anion gap in this setting. The osmolar gap should be elevated early after ingestion of an alcohol and progressively decrease as anion gap metabolic acidosis develops. This increased osmolality is due to the abundance of the osmotically active parent compound, and the acidosis is due to the production of its metabolites. When calculating the osmolar gap, it is important to include ethanol in the calculation since ethanol is also osmotically active. The equation to measure the osmolar gap is as follows:
- Serum osmolality = [2(Na) + BUN/1.6 + Glucose/18 + Ethanol/4.6]
The osmolar gap cannot be used to rule out the presence of toxic alcohol but may be useful as an indication to start treatment when the osmolar gap is greater than 25 mOsm/kg. Although, some references cite the use of an osmolar gap of greater than 50 mOsm/kg. Using the above equation, a toxic alcohol concentration can theoretically be extrapolated from the gap using the molar mass of methanol or ethylene glycol, 32 g/mol, and 62 g/mol, respectively. It should be noted that a baseline osmolality gap is believed to be within a range from -9 to 19 mOsm/kg. This should be considered when calculating the osmolar gap, and the true result of the calculation may be +/- 20 compared to the finding. Serial measurements of serum osmolality and osmolar gap calculations are not necessary or indicated in evaluation. [1]
When ethylene glycol toxicity is being considered in a patient presenting with an anion gap metabolic acidosis, the patient should be evaluated for acute renal injury. In addition, when a serum ethylene glycol concentration cannot be confirmed, it is especially important to rule out salicylate toxicity. An osmolality gap may not be significantly elevated once the patient is acidotic, as the parent compound will have already metabolized to an unknown degree, and if presenting significantly late, the osmolar gap may be normal. A 12-hour observation period should not be pursued if the patient is already acidotic; however, if stable, the patient should be checked for serum or urine ketones and treated with 1 to 2 liters of isotonic, dextrose-containing intravenous fluids. If improvement occurs as evidenced by improved acidosis and a decrease in the anion gap, then toxic alcohol ingestion should be considered less likely, and other etiologies should be more strongly considered. [1]
Oftentimes, a serum alcohol concentration can also be estimated. (Note, the term "alcohol" does not specifically refer to only ethanol). This approach may be useful in risk stratification of small, inadvertent ingestions with very clear, accurate histories. The estimation is based on the dose or amount ingested in milliliters (D), percent concentration of ingested alcohol, bioavailability (BV), the volume of distribution (V) expressed as liters per kilogram, and patient weight (W) in kilograms. This is most useful when assessing for toxicity in small, accidental ingestions, usually by children. The equation is as follows:
- Serum concentration = (D x BV)/(V x W)
This is performed by first determining the percent concentration of the ingested agent, with 1% being equal to 1 gm/100 mL. The amount ingested is then determined by multiplying the percent concentration by the volume ingested. This product is then multiplied by bioavailability, which is conservatively assumed to be 100%. This is then divided by the product of the volume of distribution (0.7L/kg) and the patient’s weight in kilograms. The result will be in grams per liter which will need to be converted to milligrams per deciliter (or multiplied by 100). The resulting serum concentration assumes that the total ingestion occurred instantaneously with complete absorption.[1] With small mouthfuls, it can be assumed that an adult’s mouthful is approximately 30 mL and a toddler’s mouthful is approximately 10 mL.[14]
Toxic alcohol exposure is confirmed when a serum concentration demonstrates the diagnosis. It should be suspected in a patient with developing metabolic acidosis with an elevated anion gap, preceded by an osmolality gap that is decreasing over time, with associated symptoms as described above.[1] Other findings that may be present in ethylene glycol toxicity may include urinary calcium oxylate crystals, urinary flourescence of excreted sodium flourescein - an occacional antifreeze additive, serum hypocalcemia secondary to precipitation of caclium oxylate crystals, QT interval prolongation on electrocardiogram as a result of said hypocalcemia, and elevated or falsely elevated lactate as a result of assay interference from glycolic acid. These findings are nonspecific and can be falsely positive or negative in this setting.
Treatment / Management
Treatment options for ethylene glycol toxicity include supportive care, fomepizole (Antizole, 4-Methylpyrazole or 4MP), ethanol, dialysis and theoretically, thiamine, pyridoxine and magnesium. Fomepizole is the antidote for toxic alcohols, and it acts by inhibiting alcohol dehydrogenase to cease toxic alcohol metabolism. Ethanol may also be utilized therapeutically to inhibit alcohol dehydrogenase when fomepizole is unavailable. There are advantages and disadvantages to either treatment. Fomepizole is more easily dosed, does not cause any inebriation, and more strongly inhibits alcohol dehydrogenase, but is fairly expensive. Ethanol is less expensive but is harder to dose accurately, requires close monitoring of the serum ethanol concentration, and causes inebriation that may necessitate intensive care monitoring.[1][15]
Indications for antidotal treatment include an elevated ethylene glycol concentration and severe or progressing acidosis, despite resuscitation, with clinical suspicion of exposure. Recommendations regarding specific ethylene glycol concentration treatment thresholds vary, with most conservative recommendations to treat if greater than 20 to 25 mg/dL. However, if metabolic acidosis is mild or not present, and there is no evidence of end-organ toxicity, particularly renal, then an ethylene glycol concentration of 62 mg/dL is an appropriate starting point for treatment as molar calculations indicate this would correlate with a maximum of 10mmol/L of a toxic metabolite. This concentration of metabolites should not alone account for more than a 10 mmol/L base deficit or a an assoicated toxic effect. (Note: the molar based treatment cutoff for methanol is 32 mg/dL; see methanol toxicity chapter). When ethylene glycol concentration is not readily available, then treatment should be initiated when bicarbonate progresses below 15mmol/L or if there is evidence of renal toxicity. After fomepizole is administered, there are 12 hours in which ethylene glycol metabolism is halted. This allows for adequate time to obtain an ethylene glycol concentration and arrange for dialysis, if needed.[16][1]
Fomepizole and ethanol inhibit alcohol dehydrogenase to stop the conversion of ethyelene glycol (and other alcohols) to its toxic metabolites. When alcohol dehydrogenase is inhibited, clearance of ethyelene glycol is prolonged from a half-life of 4-6 hours to an effective half-life of approximately 17 hours. Fomepizole is given intravenously with a loading dose of 15 mg/kg, followed by maintenance dosing of 10 mg/kg every 12 hours for four doses, or until the ethylene glycol concentration is at least less than 62 mg/dL with a normal acid-base status; however, more conservative recommendations of below 25 mg/dL exist. It is not mandatory to complete four doses. If additional dosing is required beyond four maintenance doses, then dose should be increased to 15 mg/kg every 12 hours due to fomepizole's autoinduction of its own metabolism. During dialysis, fomepizole should be administered every 4 hours as it is removed during dialysis. For a standard 4-hour dialysis session, fomepizole should be dosed both before and after the session, with resumption of 12-hour dosing thereafter.[1][16][17][7][18]
Using ethanol as an antidote is more complicated than treatment with fomepizole. It is difficult to titrate, monitor and is inebriating. Ethanol may be given intravenously or orally, but its use should be limited to the fomepizole is inaccessible. Although it is considered less expensive than fomepizole, it often carries a higher total cost during hospital stay. During treatment, the goal serum ethanol concentration is 80 to 120 mg/dL. Intravenous ethanol formulary is usually 10%, and the loading dose is calculated using the product of the goal plasma concentration (C = 100mg/dL), the volume of distribution of ethanol (V = 0.6L/kg), and the patient’s weight. Maintenance dosing is then based on elimination rate. Empirically, 10% intravenous ethanol may be administered with a loading dose of 8 mL/kg over 30 to 60 minutes, followed by maintenance dosing of 1-2 mL/kg per hour. Maintenance dosing is doubled during dialysis. Oral dosing may be calculated using the above equation for serum alcohol concentrations by using 100 mg/dL for the serum concentration and then solving for the percentage amount of ethanol ingested. Empirically, 50% (100 proof) oral ethanol may be administered with a loading dose of 2 mL/kg followed by 0.2-0.4mL/kg per hour. Maintenance dosing is doubled during dialysis.[1][11][19]
Ethylene glycol and its metabolites are dialyzable; however, with proper administration of fomepizole, dialysis is generally not indicated in the absence of renal dysfunction. In addition, dialysis can unjustifiably increase risk and cost to the patient. Unlike methanol or diethylene glycol, fomepizole alone is the recommended treatment for a toxic exposure to ethylene glycol without renal dysfunction, and only minimal acid-base disturbances, as it is far less likley that any toxicity is associated with unmetabolized ethylene glycol. The effective half life of ethylene glycol is only increased to about 17 hours when alcohol dehydrogenase is inhibited; therefore, dialysis does not necessarily decrease length of stay either. Furthermore, its use often requires being in the intensive care unit in many hospitals, thus increasing costs. Hemodialysis should be strongly considered in the presence of renal dysfunction, severe metabolic acidosis and severe electrolyte abnormalities. Normal urinary output needs to be assured to treat with fomepizole alone so that ethylene glycol can be reliably excreted. The presence of severe acidosis indicates the active and likely incomplete metabolism of ethylene glycol, with the concern that circulating glycolic acid may be converted to oxalate, which increases the risk of worsened renal function. Continuous renal replacement, although less effective, therapy may be considered if intermittent hemodialsyis is not feasible, particularly in the setting of hemodynamic instability. The decision to utilize hemodialysis is complicated and should be made in consultation with a medical toxicologist.[20][21][17][22][23]
Additional treatment options may also be considered. Sodium bicarbonate infusion may be helpful, particularly in severe metabolic acidosis, but is not universally considered a standard recommendation. Calcium gluconate may be indicated if complications occur as a result of hypocalcemia, but should otherwise be replaced cautiously and judiciously as exogenous calcium administration may enhance the precipitation of calcium oxylate crystals. Seizures in the presence of hypocalcemia should be treated with benzodiazepines. Theoretically, administration of thiamine and pyridoxine and magnesium may assist in shunting glycolic acid metabolism away from oxalic acid and toward its nontoxic metabolites, α-hydroxy-β-ketoadipic acid and glycine, respectively, utlizing the mechanism discussed in the pathophysiology section.
Admission to the intensive care unit should be considered in the presence of severe symptomatology, including obtundation, severe metabolic or electrolyte derangements. Intensive care admission should also be considered based on treatment complexity, including the use of dialysis and more importantly, if ethanol treatment is required.
Differential Diagnosis
The differential diagnosis for toxic alcohol ingestion includes any cause of metabolic acidosis. Important toxicological considerations for metabolic acidosis are salicylates, acetaminophen, iron, carbon monoxide, cyanide, alcoholic ketoacidosis, and ingestion of other alcohols, such as methanol, diethylene glycol or toluene. Ingesstion of agents contanining more than one alcohol or toxic substance should also be considered. Nontoxicological considerations should include alcoholic ketoacidosis, diabetic ketoacidosis, sepsis, and uremia.[1]
Toxicity and Side Effect Management
Mainstay of management is supportive care and treatment with fomepizole. Fomepizole is exceptionally safe with no significant adverse effects.[24] When ethanol is used as an antidote, it can be difficult to manage, requiring critical care management for close titration and intoxciation with its associated complications, such as encephalopathy and respiratory depression.[25] Dialysis carries its own risks and benefits, including decreased blood pressure, bleeding from catheter placement, and infection.
Prognosis
Complications
When patients survive ethylene glycol toxicity, there is generally recovery from any associated nephropathy; although, additional nephrology management and dialysis may be required after discharge.
Consultations
- All patients with ethylene glycol toxicity should be managed in consultation with a medical toxicologist or the local poison center.
- If hemodialysis is determined to be indicated by toxicologist, then nephrology consultation is indicated.
- If ethanol is utilized as an antidote, critical care management is recommended.
Deterrence and Patient Education
It is important to keep all antifreeze products and related substances in their labeled containers and stored out of reach of children.
Pearls and Other Issues
- Osmolar and anion gaps absolutely cannot be relied upon to rule out toxic alcohol poisoning.
- Ethylene glycol is undergoes multiple metabolic steps, with metabolites glycolic acid and oxalic acid being primarily responsible for acidosis and renal injury, respectively.
- End-organ toxicity primarily includes nephropathy secondary to the deposition of calcium oxalate crystals.
- Ethylene glycol is osmotically active while its metabolites are responsible for the associated anion gap metabolic acidosis.
- A normal osmolar gap is not reassuring and should be anticipated in the presence of an anion gap acidosis believed to be related to toxic alcohol poisoning.
- The mainstay of treatment is fomepizole, supportive care and resuscitation. However, dialysis may be indicated.
- In the absence of end-organ toxicity, ethylene glycol toxicity generally does not require dialysis.
- When patients survive and have resulting renal dysfunction or failure, recovery of renal function is the norm but may take weeks to months.
Enhancing Healthcare Team Outcomes
The importance of managing in consulation with a medical toxicologist or poison center expert cannot be overstated.
(Click Image to Enlarge)
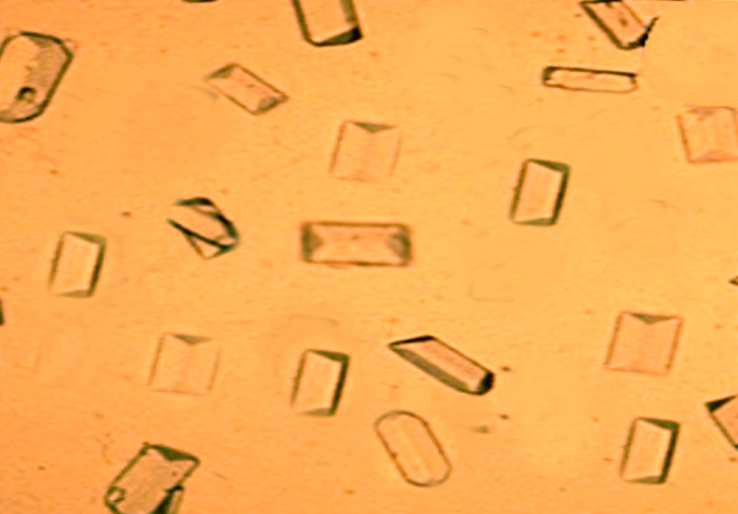
Calcium oxalate crystals in urine
Image courtesy S Bhimji MD