Anatomy, Shoulder and Upper Limb, Hand Ulnar Bursa
- Article Author:
- Ethan Sawyer
- Article Editor:
- Matthew Varacallo
- Updated:
- 8/10/2020 5:18:48 PM
- For CME on this topic:
- Anatomy, Shoulder and Upper Limb, Hand Ulnar Bursa CME
- PubMed Link:
- Anatomy, Shoulder and Upper Limb, Hand Ulnar Bursa
Introduction
Bursae are sac-like structures, lined with synovial fluid, found throughout the musculoskeletal system in locations prone to friction, such as bony prominences and areas surrounding tendons and ligaments. They create a physiologic cushion between adjacent tissues and structures to facilitate dynamic function and movement.[1] One specific subtype of bursa is a synovial tendon sheath which surrounds tendons as they pass through anatomic spaces to carry out their respective dynamic functions. The ulnar bursa is the synovial tendon sheath that surrounds and reduces the friction on the tendons of wrist and finger flexors as they pass through the carpal tunnel. The ulnar bursa consists of three distinct invaginations that surround the structures of the carpal tunnel including[2]:
- Deep layer
- Between the carpal bones and the flexor digitorum profundus tendons
- Intermediate layer
- Between the flexor digitorum profundus tendons and flexor digitorum superficialis tendons
- Superficial layer
- Volar to the flexor digitorum superficialis tendons
Structure and Function
Like other bursae, the ulnar bursa is a sac of synovial fluid that typically remains collapsed with the walls being held apart by the thin layer of fluid. It provides a means for smooth movement by reducing friction for the tendons of both the flexor digitorum profundus as well as the flexor digitorum superficialis as they pass deep to both the flexor retinaculum and the median nerve in the carpal tunnel and into the metacarpals of the hand. There are three communicating invaginations of the ulnar bursa at the level of the carpal tunnel. The most superficial invagination is between the transverse carpal ligament and the flexor digitorum superficialis tendons. The middle and deep invaginations are situated superficial and deep to the flexor digitorum profundus tendons respectively. The ulnar bursa encases these tendons until they reach the midpalmar region overlying the second, third, and fourth metacarpals but continues distally over the flexor tendons of the fifth digit and often communicates with the flexor tendon sheath of the fifth digit.[3]
Embryology
Though the development of the wrist joint has been the subject of intensive study, there is not a complete consensus as to the precise origin, development, and organization of the various elements of the wrist joint, including the ulnar bursa. However, the synovial membranes of the wrist joint have been shown to develop from the intermediate layer interzonal mesenchyme around week 13 of development.[4]
Blood Supply and Lymphatics
The proximal portion of the ulnar bursa in the carpal region receives its arterial supply from small branches of both the radial and ulnar arteries. The distal portion of the bursa overlying the metacarpals receives vascular by both the superficial and deep palmar arches.[5] However, it bears mentioning that bursae are typically not well vascularized.[1] The lymphatic vessels of the hand and forearm ascend the arm proximally coursing with superficial veins like the basilic vein and travel to the cubital lymph nodes adjacent to the medial epicondyle of the humerus. The lymphatic vessels traveling superficially near the cephalic vein drain to the apical axillary lymph nodes primarily, however, the deltopectoral lymph nodes are another minor drainage site. The deep lymphatic vessels accompany the deep veins and drain into the humeral axillary lymph nodes and then the subclavian lymphatic trunk.[6]
Nerves
The location of the ulnar bursa is on the anteromedial side of the wrist and hand which receives its innervation from the ulnar nerve.
Muscles
The ulnar bursa encases the tendons of the flexor digitorum profundus and the flexor digitorum superficialis muscles in the carpal tunnel.
Physiologic Variants
The ulnar bursa typically originates at the level of the pronator quadratus and continues distally to approximately 1 to 3 cm proximal to the flexor tendon sheaths of digits two, three, and four. However, studies have shown communication between the ulnar bursa and the flexor tendon sheaths of digits two, three, and four at rates of 5.1%, 4%, and 3.5% respectively.[7] Communication with the flexor tendon sheath of the fifth digit is much more common, occurring in 50 to 80% of cases.[3] Another potential communication with the ulnar bursa is the radial bursa. The radial bursa, which encases the flexor pollicis longus, has shown to have intercommunications with the ulnar bursa in up to 50% of cases. These communications are made by intermediate bursae which have been described posterior to the deep flexor tendon of the second digit as well as between the superficial and deep flexor tendons of the second digit.[8]
Surgical Considerations
With the ulnar bursa’s location deep to the flexor retinaculum of the wrist, surgeons frequently encounter it during hand and wrist surgeries, including carpal tunnel release operations. Carpal tunnel releases are the most common hand and wrist surgeries in the United States with more than 400000 procedures annually.[9] The parietal surface of the ulnar bursa is adherent to the flexor retinaculum which typically results in the incision of the synovial sheath as the surgeon cuts through the flexor retinaculum. One trial studied the difference in functional and symptomatic outcome in carpal tunnel release with preservation of the ulnar bursa against the standard operation in which there is incision of the bursa. The study found no significant difference in grip strength or self-reported symptoms between the two groups. The study noted that preservation of the ulnar bursa made visualization of the median nerve more difficult during the operation.[10]
If the ulnar bursa becomes infected, which most commonly occurs through a spread from communicating flexor tendon sheaths in the hand, prompt irrigation and debridement are necessary, in addition to intravenous antibiotics.[11]
Clinical Significance
Carpal tunnel syndrome is a common disorder caused by inflammation of the median nerve[12]. The pathophysiology is often idiopathic, however, many cases are thought to be due to the fibrous hypertrophy or increased volume of the ulnar bursa adjacent to the nerve, which can irritate the nerve which is confined superiorly by the flexor retinaculum of the wrist.[13] This hypertrophy is often secondary to repetitive wrist flexion. There is an increased prevalence of carpal tunnel syndrome in obese and pregnant patients as well as those with hypothyroidism and congestive heart failure. This increased incidence is theorized to be secondary to an increase in synovial fluid volume which may be present in these groups of patients.[14]
Bursitis, the painful swelling of a bursa as a result of noxious stimuli, can occur in the ulnar bursa but is more frequent in the bursa overlying bony protuberances such as the subacromial bursa or the trochanteric bursa.[1] Septic bursitis of the ulnar bursa can occur and is most often the result of the spread of pyogenic flexor tenosynovitis from the flexor tendon sheaths of the fingers to the ulnar bursa. The most common synovial communication with the ulnar bursa is the flexor tendon sheath of the fifth digit, though any anomalous synovial channels have the potential to spread infection from their sheath to that of the ulnar bursa.[14] Septic bursitis can be the result of invasive procedures and the most common bacteria implicated in septic bursitis is Staphylococcus aureus.[1]
Other Issues
Though rare, extrapulmonary tuberculosis can infect the musculoskeletal system and reports exist of cases of tuberculous tenosynovitis.[15]
(Click Image to Enlarge)
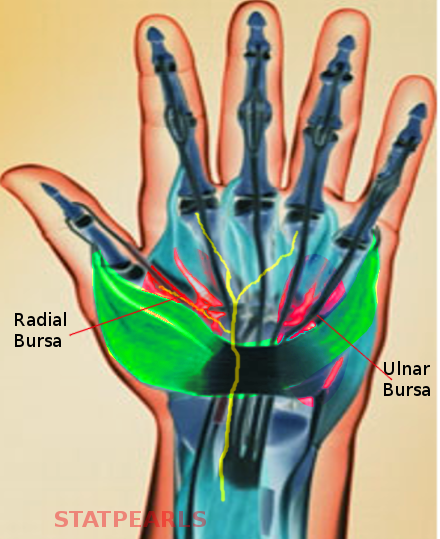
Ulnar bursa
Image courtesy S Bhimji MD