Neuroanatomy, Nucleus Vestibular
- Article Author:
- Elizabeth Hernandez
- Article Editor:
- Joe M Das
- Updated:
- 10/27/2020 8:32:57 AM
- For CME on this topic:
- Neuroanatomy, Nucleus Vestibular CME
- PubMed Link:
- Neuroanatomy, Nucleus Vestibular
Introduction
The vestibular nuclei are located in the medulla and pons of the hindbrain. It is a complex composed of four major nuclei that integrate information from the primary vestibular afferents, contralateral nuclei, somatosensory organs, and the cerebellum. The vestibular complex projects fibers to the contralateral vestibular nuclei, spinal cord, cerebellum, thalamus, and the motor nuclei of the extraocular muscles. The major vestibular nuclei are highly interconnected with many overlapping functions. It plays an essential role in maintaining equilibrium, posture, head position, and clear vision with movement. This article discusses the main structural, functional, and nervous connections of the four major nuclei.
Structure and Function
The vestibular nucleus spans from the rostral medulla to the caudal pons. It is located bilaterally along the floor of the fourth ventricle and is lateral to the sulcus limitans.[1][2] The complex extends this length in two major columns, medial and lateral.
The vestibular complex subdivides into four major nuclei:
- Lateral vestibular nucleus (LVN)
- Medial vestibular nucleus (MVN)
- Superior vestibular nucleus (SVN)
- Descending (inferior) vestibular nucleus (DVN)
- LVN - The LVN, also known as Deiter’s nucleus, extends along the lateral column of the vestibular complex. It is bordered by the SVN, MVN, and DVN. Lateral to the LVN are the sensory fibers of CN VIII.[3] It is distinguishable from the other nuclei by its giant cells in the dorsocaudal region and intermediate-sized cells in the rostroventral region.[2] The LVN functions to aid in the vestibulospinal reflex to maintain proper posture and balance via the paravertebral extensor muscles and proximal extensor muscles of the limbs.[1]
- MVN - The MVN, also known as the nucleus of Schwalbe, is the largest of the four nuclei in total cell volume and, unlike the others, runs mostly in the medial column.[3] It is bordered by the SVN and DVN, as well as posteriorly by the fourth ventricle and inferiorly by the dorsal motor vagal nucleus and hypoglossal nucleus. The MVN has a dorsal collection of small, parvocellular neurons and a ventral collection of larger, magnocellular neurons.[2] It mediates the vestibulo-ocular reflex (VOR) along with the SVN, which ensures clear vision by rotating the eyes opposite to the head during horizontal rotation.[1] For example, if the head is turned quickly to the right, both eyes turn toward the left. It also functions to control head and neck movements to maintain balance via the medial vestibulospinal tract.[4]
- SVN - The SVN, also known as the nucleus of Bechterew, extends along the lateral column in an elongated, elliptical form. It is the most rostral of the vestibular nuclei. It is bordered ventral-laterally by the LVN, dorsally by the superior cerebellar peduncle, and medially by the fourth ventricle. Additionally, it also merges with the trigeminal nucleus ventrally.[3] This elliptical shaped nucleus has a uniform distribution of medium-sized cells. It functions to aid in coordination and postural adjustments, as well as related eye movements. It appears to play a role in the conscious perception of gravity and movement.[2]
- DVN - The DVN is the most caudal of the nuclei and is neighbored superiorly by the LVN, medially by the MVN, posteriorly by the lower end of the fourth ventricle, and anteriorly by the reticular formation.[3] On microscopic examination, the DVN seems less densely populated than the other nuclei due to its characteristic longitudinal fiber bundles.[2] It receives information about head tilt and gravity, which consequently affects blood flow, respiratory rate, and heart rate upon standing.[2]
Embryology
The nervous system develops from the ectoderm of the trilaminar embryo. From there, the neural plate folds and forms the neural tube. The rostral neural tube divides and forms the three primary vesicles (prosencephalon, mesencephalon, and rhombencephalon). The rhombencephalon (or hindbrain) divides into the metencephalon (pons and cerebellum) and the myelencephalon (medulla oblongata). The vestibular nuclei develop within both the metencephalon and the myelencephalon.[5]
The developing hindbrain creates two longitudinal columns of neurons that receive fibers from the vestibular part of the ear. These longitudinal columns subdivide into functionally specified rhombomeres (the transverse boundaries), derived from the rhombic lip. The rhombic lip is known as the source of migratory cell populations that give rise to the major dorsal and ventral nuclei in the hindbrain. Vestibular nuclei form from several of these rhombomeres and are highly analogous across vertebrates, from fish to humans.[6][7]
Blood Supply and Lymphatics
The primary vascular supply to the vestibular nucleus is the posterior inferior cerebellar artery (PICA), a branch of the vertebral artery.[8]
Nerves
Vestibular nuclei interconnect via commissural projections with their homologous and non-homologous vestibular nuclei; this allows for the comparison of activity on both sides.[9] All four of the major vestibular nuclei receive input from the entire or parts of the peripheral vestibular apparatus via the vestibular portion of cranial nerve (CN) VIII, the vestibulocochlear nerve.[10]
- LVN - The LVN receives input from the vestibulocerebellum and all parts of the vestibular apparatus. Fibers from the vestibulocerebellum, also known as the flocculonodular lobe, convey information about head tilt and gravity.[10] Efferent fibers from the LVN primarily regulate the lateral vestibulospinal tract, with lesser projections from the DVN. These fibers descend via the ipsilateral ventral horn of the spinal cord and extend the length of the cord, providing input to motor interneurons for the extensor muscles of the back and extremities for their respective side. The lateral vestibulospinal tract has excitatory effects on extensor motor neurons and some inhibitory effects on flexor motor neurons.[11]
- MVN - The MVN primarily receives afferent fibers from the lateral semicircular canals. Ascending fibers leave the MVN and cross the midline via the medial longitudinal fasciculus (MLF). They then innervate the contralateral paramedian pontine reticular formation (PPRF) and contralateral motor nuclei of the extraocular muscles (CN III, IV, and VI). This pathway mediates the VOR, which is important for clear vision during vertical and rotational movements.[4][12] Additionally, fibers that make up the medial vestibulospinal tract primarily originate from the MVN. From there, these fibers descend via the ipsilateral ventral horn of the spinal cord. They terminate in the cervical and upper thoracic spinal cord levels and provide input to motor interneurons.[11] Lastly, the MVN projects to several parts of the cerebellum, including the flocculonodular lobe and the anterior and posterior vermis.[2]
- SVN - The SVN receives afferent information from the superior and posterior semicircular canals. Efferent fibers from the SVN combine with fibers from the DVN to travel to the fastigial nuclei within the flocculonodular lobe of the cerebellum. The flocculonodular lobe is involved in balance maintenance and is necessary for adaptation to reflexive eye movements. The SVN also sends fibers to the nuclei of the thalamus.[2]
- DVN - The DVN receives afferent fibers from otolith organs (the utricle and saccule) of the inner ear. The DVN has projections to the other three vestibular nuclei and the cerebellum.[1] Descending projections from the DVN and MVN modulate vestibulo-sympathetic reflexes, which affect blood flow, respiratory rate, and heart rate. Additionally, both the medial and lateral vestibulospinal tracts have fibers that originate in the DVM.[2]
Muscles
The vestibular nuclei have terminal effects on extraocular muscles and postural muscles of the back, neck, and extremities.[2]
Physiologic Variants
The vestibular apparatus and, correspondingly, vestibular nuclei have remained highly unchanged across vertebrates.[7]
Surgical Considerations
During cochlear implantation, a procedure used to restore hearing in patients with severe hearing loss, the cochlea and vestibular organs may be damaged. This damage can lead to vestibular symptoms of spontaneous nystagmus and vertigo. In time, the activity of the vestibular nucleus has shown correlations with increased compensation and plasticity, with a spontaneous decrease in central vestibular symptoms. Therefore, vestibular function testing may be important before the procedure and careful surgery considered in patients with functional vestibular organs.[13]
Clinical Significance
Acute Unilateral Vestibular Loss
While the cause of acute vestibular dysfunction correlates with reactivation of a viral infection, it is unknown. However, unilateral loss of function of the vestibular nucleus is the most severe condition that occurs within the vestibular apparatus. The decrease in the firing rate of the compromised side causes a permanent rotation of the head to the healthy side, causing a slow-phase drift of the eyes toward the side of the lesion, with a rapid quick-phase eye movement back towards the healthy side.
Clinically, this leads to horizontal-torsional nystagmus, rotational vertigo, and postural imbalance. The direction of the quick-phase characterizes the direction of the nystagmus. For example, a leftward quick-phase would be left-beating nystagmus. The imbalance and characteristic spontaneous nystagmus resolve within days to weeks due to restoration of activity in the lesioned side.[14][15]
Wallenberg Syndrome
Wallenberg syndrome, also known as the lateral medullary syndrome, is due to an occlusion of the vertebral artery or the PICA. The PICA supplies the medial portion of the posterior cerebellum and the posterolateral medulla, which includes the vestibular complex.[16] It typically occurs in a patient with hypertension, diabetes, or smoking history. Following ischemia of the vestibular nuclei, the patient usually presents with vertigo, ipsilateral nystagmus, nausea, and vomiting. Vertigo is the sensation of rotation or movement of the body or environment, and patients commonly describe it as the feeling that “the room is spinning.”
The involvement of the cerebellum leads to ipsilateral ataxia and falling toward the affected side. The involvement of other parts of the medulla leads to dysphagia, hoarseness, and ipsilateral Horner syndrome. On the contralateral side, the patient may present with spinothalamic sensory loss and mild hemiparesis.[17][18]
(Click Image to Enlarge)
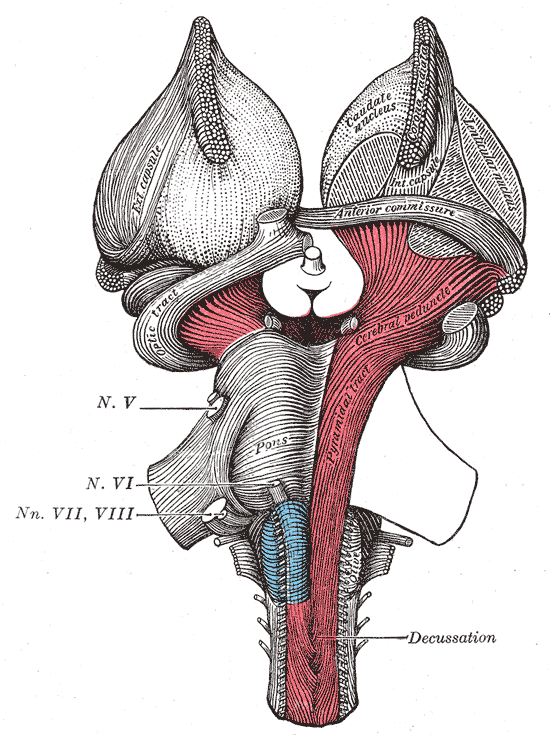
The Hind-brain or Rhombencephalon, Superficial dissection of brain-stem. Ventral view, Cranial Nerve, Pons, Caudate nucleus, Anterior commissure, Cerebral peduncle
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)

The Hind-brain or Rhombencephalon, Dissection of brain-stem; Dorsal view, Stria terminalis, Auditory radiation, Medial geniculate, Inferior colliculus, Inferior Peduncle Nucleus cinerea; cuneatus; gracilis, Nucleus spinal tract; trigeminal
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)
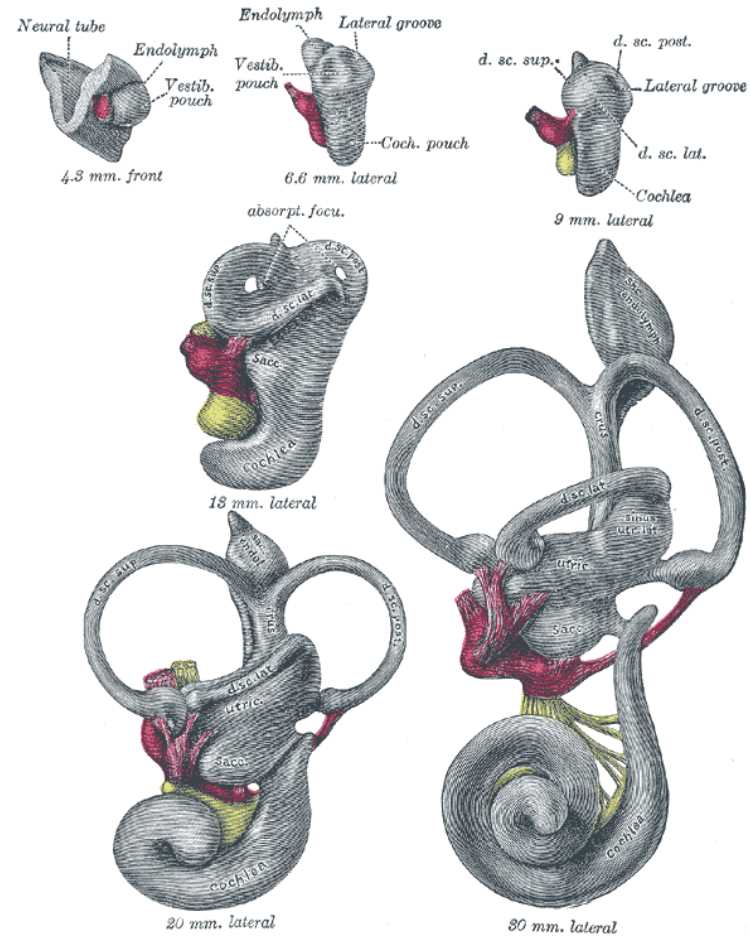
Vestibular System, semicircular canals
Contributed by William Gossman Collection