Anatomy, Shoulder and Upper Limb, Distal Radio-Ulnar Joint
- Article Author:
- Daniel Arias
- Article Editor:
- Matthew Varacallo
- Updated:
- 7/31/2020 3:57:23 PM
- For CME on this topic:
- Anatomy, Shoulder and Upper Limb, Distal Radio-Ulnar Joint CME
- PubMed Link:
- Anatomy, Shoulder and Upper Limb, Distal Radio-Ulnar Joint
Introduction
The distal radioulnar joint (DRUJ) is responsible for the integrity of the articulation between the distal radius and distal ulna; this is important in both supination and pronation of the forearm, as well as anteroposterior translational stability. The distal radioulnar joint is a critical stabilizing structure of the ring stabilizing the radius and ulna, and pathologies afflicting the distal radioulnar joint can impact not only the hand and wrist but the elbow as well. Clinically, the distal radioulnar joint carries critical importance as it can undergo an acute injury or chronic degeneration as a result of long-term sequelae from previous injuries. This spectrum of pathology leads to significant wrist pain, dysfunction, degeneration, and subtle to gross instability. The goal of this article is to provide an anatomic review, as well as basics of clinical importance for the education of current and future healthcare providers.
Structure and Function
The distal radioulnar joint (DRUJ) formes from volar and dorsal radioulnar ligaments (RULs) and the triangular fibrocartilagenous complex (TFCC). The latter components consist of individual anatomic structures including the central articular disc, meniscal homolog, the ulnolunate and ulnotriquetral ligaments, the extensor carpi ulnaris tendon sheath/floor, and part of the joint capsule. The primary role of the distal radioulnar joint is to stabilize the articulation of the radius around the stationary ulna during pronation and supination.
Beginning with osteology, the ulnar head sits within the sigmoid notch of the radius. An anatomic study of this osseous anatomy revealed that the length of the sigmoid notch increases from volar to dorsal. There is additionally significant variation of the ulnar length, which was found to have a negative correlation to the mid-coronal length of the sigmoid notch. Obliquity of the distal radioulnar joint was also found to correlate with the ulnar variance. In patients with a typical negative ulnar variance, the sigmoid notch was found to angled in a proximal-ulnar direction, but as ulnar variance became more positive, this became progressively less angled, eventually resulting in a reverse obliquity. There was considerable variability found between the specimens analyzed, but bilateral consistency in a given specimen. This variability indicates that comparison may be made within a particular patient but should be made with caution when comparing anatomy between patients.[1]
Concerning ligamentous components, the radioulnar ligaments are the major stabilizers of the distal radioulnar joint. These are proximal condensations of the triangular fibrocartilage complex. The current school of thought states that during pronation, the dorsal radioulnar ligament becomes tight while the palmar radioulnar ligament becomes lax; during supination, the inverse occurs. Though some debate surrounds the role of ligamentous stability to the distal radioulnar joint, a growing body of evidence supports this model. Several studies have also looked into the role of the radioulnar ligaments in the translational stability of the distal radioulnar joint. These studies have agreed that dorsal radioulnar ligament is of particular importance to dorsal translational stability when the forearm is in pronation. The palmar radioulnar ligament correlates with the stability of volar translational stability with the forearm in supination. Additionally, radioulnar ligament disruption was found to increase the rotational range of motion in the biomechanical study performed by Ward, et al. This is a novel report and indicates the importance of the ligamentous complexes to the rotational stability of the distal radioulnar joint.[2]
The role of the interosseous membrane, joint capsule, and articular disc in maintaining joint stability have been less well studied but are part of the sectioning sequences used in biomechanical studies and have not consistently correlated to gross instability of the joint.
Embryology
While a great deal of embryologic investigation has occurred relative to the triangular fibrocartilagenous complex, studies targeting other ligamentous structures of the wrist are lacking. There are reports that the ligamentous structures begin to appear in O’Rahilly stage 23 embryos and are complete by the week 14 of gestation.
The Interzone is a portion of the condensed mesenchymal structure whose appearance signals the beginning of wrist joint formation. The Interzone forms three layers of which the intermediate layer is thought to be most important to the formation of the ligamentous structures of the wrist.[3]
Blood Supply and Lymphatics
Arterial supply to the distal radioulnar joint derives primarily from palmar and dorsal branches of the anterior interosseous artery. These arteries branch at the proximal border of pronator quadratus and form an anastomotic complex. Other contributions are made by anastomoses as follows: dorsal interosseous artery to the dorsal branch of the anterior interosseous artery, ulnar artery to the palmar branch of the anterior interosseous artery, and collateral circulation from dorsal and palmar carpal arches.[4][5][6]
The lymphatic pathways of the upper extremity have been poorly described, but a variety of courses have been noted, including perforators accessing the wrist compartment. These drain from distal to proximal and have little consistency in their flow from deep to superficial or superficial to deep. Primary lymph node collections in the upper extremity appear in the cubital and axillary regions.[7]
Nerves
Muscles
The flexors and extensors of the wrist, hand, and fingers provide additional soft tissue support and stabilization to the distal radioulnar joint. Of particular note is pronator quadratus. Biomechanical analysis has shown that PQ has a role in tensioning the distal radioulnar joint. Both the deep and superficial heads of pronator quadratus originate from the dorsoulnar aspect of the ulna and attach to the palmar aspect of the radius. This orientation allows for tensioning of the distal radioulnar joint during pronation, preventing interposition of the capsule and joint diastasis.[12]
Physiologic Variants
There is significant physiologic variance that occurs with ulnar length relative to the radius, as discussed in the structure and function section of this article; this results in a considerable variation of the sigmoid notch as well. There is potential significance to this variance and should merit consideration when assessing a patient with a forearm fracture or wrist pain.[1]
Surgical Considerations
Surgery is indicated for patients with isolated or associated injuries yielding significant distal radioulnar joint instability.
Surgical repair of the distal radioulnar joint is contraindicated for patients with other evident pathology including radial and ulnar length discrepancies, distal radioulnar joint arthritis, sigmoid notch incompetence, extensor carpi ulnaris tendon subluxation, or other apparent reason for wrist pain. Reconstruction of the triangular fibrocartilage complex and distal radioulnar joint often does not itself restore stability to the joint and careful patient selection should be carried out with the understanding that these procedures are performed primarily as adjunctive procedures to control pain. Various surgical reconstruction procedures exist in the literature, including reconstruction of the radioulnar ligaments, placement of an extrinsic radioulnar tether, and creating a radiocarpal sling or tenodesis. All of these procedures have their inherent limitations but have been found to help control symptoms.[13]
Clinical Significance
Distal radioulnar joint instability may result from traumatic injury or chronic degeneration. These carry varying significance and treatment options, as discussed in the surgical considerations section of this article. Chronic tears should be suspected in older patients, while acute tears occur in the setting of upper extremity trauma. Injuries to the distal radius and fractures of the ulnar styloid are often implicated in these traumatic injuries to the distal radioulnar joint. The clinical importance of these injuries is a matter of debate, and functional outcomes more than likely correlate with appropriate treatment of radial fractures than treatment of ligamentous or ulnar styloid fractures. Evaluation of distal radioulnar joint instability should include a thorough history and physical exam, including use of the piano key and press tests. The piano key test is when the examiner has the patient pronate the forearm and applies a volar force to the ulnar head, with a positive test indicated by increased translation when compared to the contralateral extremity. The press test is when the examiner has the patient pronate both forearms and press into a table. A positive test presents with the volar translation of the ulnar head. Most patients can undergo management with nonoperative therapy, including wrist and forearm strengthening, as well as functional bracing.[14]
Subluxation related ulnar neuropathy (SUN) syndrome is a potential complication of chronic instability of the distal radioulnar joint. Compression and kinking of the ulnar nerve can occur within the Guyon canal leading to numbness and tingling of the fourth and fifth digits with potential weakness of the intrinsic muscles of the hand in more advanced cases. Evaluation of symptoms of ulnar neuropathy should include stressing of the distal radioulnar joint to verify the etiology of the condition.[15]
(Click Image to Enlarge)
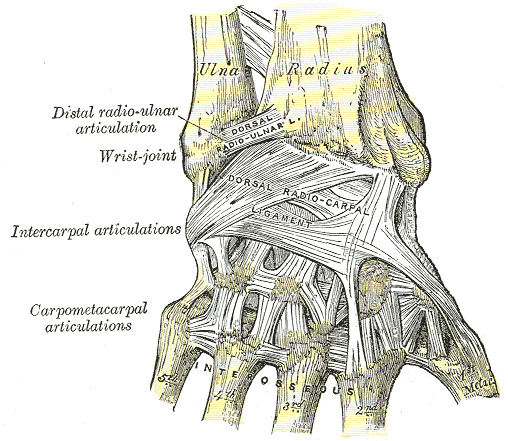
Ligaments of Wrist, Wrist, Posterior Aspect, Ulna, Radius, Distal radio-ulnar articulation, Wrist joint, Intercarpal articulations, Carpometacarpal articulations, Dorsal radioulnar ligament, Dorsal radio-carpal ligament, Interosseous, Metacarpal,
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)

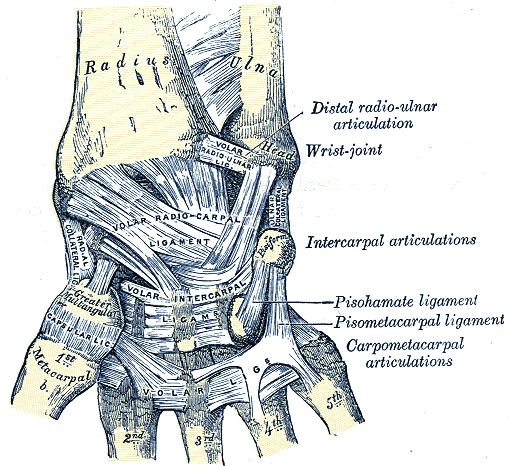
Synovial Cavities, Distal radioulnar articulation, Articular disc, Wrist joint, Radial collateral ligament, Ligament, Pisiform, Ulna, Radius, Metacarpals, Navicular, Lunate, Capitate, Hamate, Trapezium, Trapezoid, Triquetrum, Cavities
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)
Distal radioulnar joint
Contributed by Henry Gray (1918) Anatomy of the Human Body https://commons.wikimedia.org/wiki/File:Gray334.png