Anatomy, Shoulder and Upper Limb, Forearm Muscles
- Article Author:
- Brittney Mitchell
- Article Editor:
- Lacey Whited
- Updated:
- 8/15/2020 11:35:56 PM
- For CME on this topic:
- Anatomy, Shoulder and Upper Limb, Forearm Muscles CME
- PubMed Link:
- Anatomy, Shoulder and Upper Limb, Forearm Muscles
Introduction
The forearm of the upper extremity runs from the elbow to the wrist. Two bones, the radius laterally and the ulna medially, form the forearm. It has two compartments, the anterior (flexor) and posterior (extensor). The two compartments together have twenty muscles.
Structure and Function
The muscles of the forearm or antebrachium work together to move the elbow, forearm, wrist, and digits of the hand. They fall into two categories: intrinsic and extrinsic muscles. The intrinsic muscles function to move the forearm by pronating and supinating the radius and ulna. The extrinsic muscles flex and extend the digits of the hand. One muscle, the brachioradialis, traverses the elbow joint, running from the arm to the wrist, helping to flex the elbow.
Embryology
The skeletal muscles of the limbs are formed from myoblasts that migrate to the developing bones after epitheliomesenchymal transformation. During this transformation, the somatic mesoderm of the ventral somite responds to molecular signals causing migration to the developing limb bud. Once the cells have moved to their final location, the notochord, and neural tube release peptides that induce further migration and growth.
Blood Supply and Lymphatics
As the brachial artery runs down the arm and passes through the elbow, it divides into two terminal branches: the radial artery and the ulnar artery. These two arteries provide the blood supply for the entire forearm and hand.
The radial artery gives off the recurrent radial branch just distal to the radial head and traverses back up to the arm to form an anastomosis with the radial collateral of the deep brachial artery. The recurrent radial branch provides the blood to the supinator and the brachioradialis muscle. The radial artery then continues down through the forearm to the wrist where is wraps posteriorly before diving into the hand.
Similarly, the ulnar artery gives off two recurrent branches, the anterior and posterior, as it passes the elbow. These two turn upward and create anastomoses with the inferior and superior collateral arteries that branch off the deep brachial artery. The anterior ulnar recurrent artery provides blood to the pronator teres and brachialis, while the posterior ulnar recurrent artery provides blood supply to the proximal portions of the flexor muscles, bones, and elbow joint. After giving off the recurrent branches, the ulnar artery gives rise to the common interosseous branch, which will continue to divide into the anterior and posterior interosseous arteries. The names of these arteries denote which side of the interosseous membrane they run on. The anterior interosseous branch supplies blood to the muscles of the flexor compartment. As it travels down the forearm, it will eventually pierce the interosseous membrane and anastomose with the posterior interosseous artery, which is the blood supply for the extensor compartment of the forearm.
The venous system for the forearm comprises superficial and deep veins. The deep veins compose a plexus that run with the arteries described above. The major superficial veins include the basilic vein (runs on the medial side of the forearm), the cephalic vein (runs on the lateral side of the forearm), and the median vein (runs up the forearm to the median antecubital vein and drains the hand).
Nerves
The three main nerves of the forearm are the median, ulnar, and radial nerves. There are also three nerves that innervate the skin (medial, lateral, and posterior cutaneous nerves). All of these nerves branch from the brachial plexus in the axillary region of the arm and traverse down the upper extremity to the hand. The median and ulnar nerve provide the innervation for the muscles of the flexor compartment while the radial nerve provides innervation for the extensor compartment.
The median nerve gives off one main branch known as the anterior interosseous nerve. It innervates the flexor pollicis longus, part of the flexor digitorum profundus, and multiple muscular branches that go directly to muscles of the flexor compartment. The ulnar nerve does not have any terminal branches until it reaches the hand, but it does give off muscular branches as it goes down the forearm that will supply the flexor carpi ulnaris and the medial side of the flexor digitorum profundus. The radial nerve gives off the posterior interosseous nerve, which supplies the supinator and extensor carpi radialis brevis.
Muscles
There are twenty muscles of the forearm. Again, the area is split into the anterior (flexor) and posterior (extensor) compartments and then each of those is divided into superficial and deep compartments.
The superficial compartment of the flexor surface of the forearm contains the pronator teres, the flexor carpi radialis longus, the palmaris longus, the flexor carpi ulnaris, and the flexor digitorum superficialis. All of these muscles originate primarily from the medial epicondyle of the humerus. The final attachment site for the pronator teres is the middle portion of the radius. Both the flexor carpi radialis and flexor carpi ulnaris insert on the bases of the second and fifth metacarpals, respectively.[1] The flexor digitorum superficialis crosses the wrist through the carpal tunnel and inserts at the proximal interphalangeal joint at the base of the middle phalanx of digits two through five.
In the deep compartment of the flexor side of the forearm, you will find the flexor digitorum profundus, the flexor pollicis longus, and the pronator quadratus. Both the flexor digitorum profundus originates on the proximal three-fourths of the ulna, and the flexor pollicis longus originates on the anterior radius. The flexor digitorium profundus runs with the tendons of the flexor digitorum superficialis and the median nerve through the carpal tunnel to insert on the distal phalanx of digits two through five in the hand.[2] The pronator quadratus originates on the distal anteromedial ulna and inserts on the distal anterolateral radius. It allows for pronation of the forearm.
The brachioradialis resides in the superficial extensor compartment of the forearm. It originates at the lateral supracondylar ridge of the humerus and it attaches on the flexor side of the wrist immediately proximal to the radial styloid.[3] The other muscles of the superficial compartment of the extensor side of the forearm are the extensor carpi radialis brevis, extensor carpi radialis longus, extensor digitorum, extensor digiti minimi, extensor carpi ulnaris, and anconeus. These muscles find their origin from the lateral epicondyle of the humerus.
The extensor carpi radialis longus and brevis attach to the proximal portion of the second and third metacarpals. The tendons of the extensor digitorum run under the extensor retinaculum and divide to attach to the extensor hoods of the middle and distal phalanx of each of the digits two through five. The extensor digiti minimi runs along with the extensor digitorum and inserts into the extensor hood of the fifth digit. The deep compartment of the extensor side of the forearm contains the adductor pollicis longus, the extensor pollicis longus and brevis, the extensor indicis, and the supinator. Three of the muscles originate from the ulna, the adductor pollicis longus, the extensor pollicis longus, and the extensor indicis. These three muscles extend into the dorsum of the hand and attach to the digits. The adductor pollicis longus connects at the base of the first metacarpal and to the trapezium of the wrist. The extensor pollicis longus runs along the forearm to the wrist where it makes a sharp turn at Lister’s tubercle and finally attaches to the distal phalanx of the thumb. Extensor indicis runs with the extensor digitorum tendon and joins the second digit at the extensor hood. Extensor pollicis brevis and the supinator originate from the radius. Extensor pollicis brevis runs with the abductor in the forearm and connects to the base of the proximal phalanx of the first digit. The supinator is unique because it starts on the lateral epicondyle of the humerus along with the radius before wrapping around the back of the arm to connect to the radius at the same location at pronator teres. This muscle allows for the supination of the forearm.[4]
Physiologic Variants
There are multiple physiological variants of these muscles. Many of them are a function of where the muscles originate or insert. Some variations include the muscles not being present at all, which is especially true for the palmaris longus, considered a vestigial structure and approximately 14% of the population only has one or neither of these muscles.[5][6]
As with any nerve, artery, or vein, the path that it takes and its specific supply is based on the growth pattern of the individual. One of the main variations in the nerves is the Martin-Gruber connection, which forms in the forearm when the median nerve sends a branch to join with the ulnar nerve as it passes deep to the flexor digitorum superficialis. This occurs in approximately 17% of the population and leads to some median nerve innervations in the intrinsic muscles of the hand.[7]
Surgical Considerations
If any of the nerves, arteries, veins, tendons, or muscles of the forearm are lacerated, a surgeon (vascular or orthopedic) should be consulted to repair the damage.
Compartment syndrome is also another notable surgical consideration. This syndrome occurs when swelling of the area compresses the vessels and nerves in the region. The most common cause is fractures of the bones of the forearm. Signs and symptoms of this condition are pain out of proportion to exam, pallor, paresthesias, pulselessness, and paralysis. If compartment syndrome is on the differential, the examiner should evaluate compartment pressures. A pressure between 30-45mmHg indicates compartment syndrome. If the patient has unequivocally positive findings on physical exam, surgeons may forgo getting compartment pressures and initiate treatment of the problem. The procedure of choice to relieve compartment syndrome is a fasciotomy, a surgical procedure where the skin is cut to open all compartments of the forearm to release the tension created by the swelling.[8]
Clinical Significance
During a neurologic exam, the tendon of the brachioradialis is used to test C7.
The anatomical snuffbox, which has as its boundaries the tendons of the extensor pollicis longus, the extensor pollicis brevis, and the abductor pollicis, is also a point of significance. If a patient falls on their outstretched hand and has tenderness over the anatomical snuffbox, it can be difficult to differentiate between a strain of the muscles/tendons and a scaphoid fracture. Even if there is no evidence of a scaphoid fracture on x-ray, these patients should be put into a thumb spica splint and followed up in two weeks for repeat x-rays.[9]
(Click Image to Enlarge)
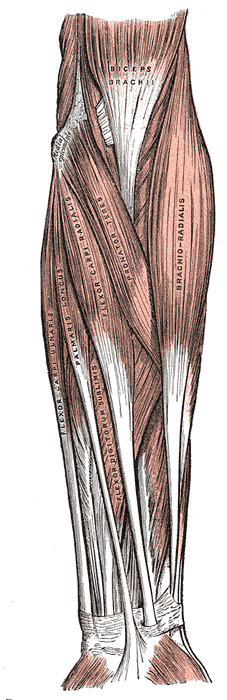
Muscles and Fascia of the forearm, Biceps Brachii, Brachioradialis, Pronator Teres, Flexor Carpi radialis, Palmaris longus, Flexor carpi ulnaris, Flexor digitorum sublimis,
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)
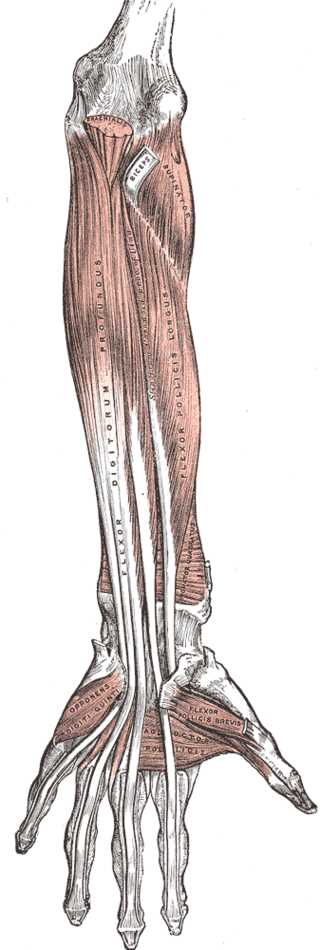
Muscles and Fascia of the Forearm, Brachialis, Biceps, Supinator, Flexor digitorum profundus, Flexor pollicis longus, opponens digiti quinti, Adductor pollicis, Flexor pollicis brevis
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)
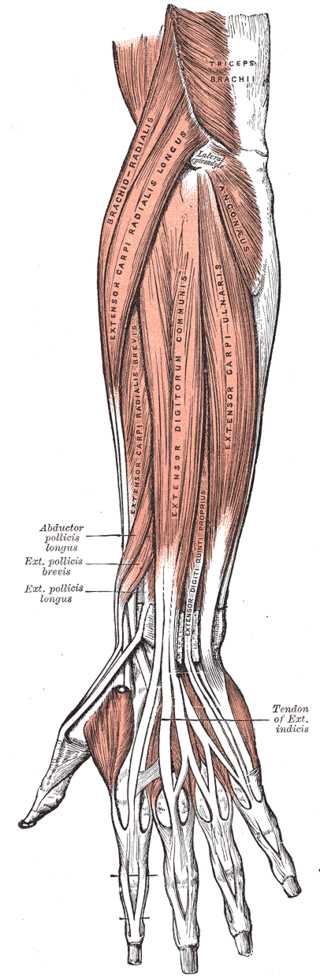
Anterior view of the Muscles and Tendons of the Forearm
Contributed by Gray's Anatomy Plates