Anatomy, Shoulder and Upper Limb, Hand Bones
- Article Author:
- Daniel Arias
- Article Editor:
- Matthew Varacallo
- Updated:
- 7/31/2020 3:57:27 PM
- For CME on this topic:
- Anatomy, Shoulder and Upper Limb, Hand Bones CME
- PubMed Link:
- Anatomy, Shoulder and Upper Limb, Hand Bones
Introduction
Each hand consists of 27 bones. The osseous anatomy of the human hand is integral to its impressive functionality. The purpose of this article is to provide a review of hand osteology for the education of current and future healthcare providers.
Structure and Function
The carpus (proximal and distal rows), metacarpal bones, phalanges, and various sesamoid bones form the skeletal hand.[1][2] There are five metacarpals, fourteen phalanges, and four consistently present sesamoid bones in the hand.
The wrist connects to the hand at the carpometacarpal (CMC) joints.[3] The first CMC forms from the articulation between trapezium and base of the first metacarpal. The base of the second metacarpal articulates with trapezium, trapezoid, and capitate. The base of the third metacarpal articulates with capitate. The base of the fourth metacarpal articulates with capitate and hamate. The fifth metacarpal's base articulates with the hamate.[4][5]
The first metacarpal bone corresponds to the thumb, the second to the index finger, the third to the long finger, the fourth to the ring finger, and the fifth to the small finger. The thumb has two phalanges, named proximal and distal phalanges. The proximal phalanx base forms the metacarpophalangeal (MCP) joint with the first metacarpal head.[6] The head of the proximal phalanx articulates with the base of the distal phalanx to form the interphalangeal (IP) joint. The index, long, ring and small fingers each have proximal, middle, and distal phalanges. The proximal phalanges form MCP joints with their respective metacarpal bones. The head of each proximal phalanx articulates with the base of each middle phalanx to form proximal interphalangeal (PIP) joints. The head of each middle phalanx articulates with the base of each distal phalanx to form distal interphalangeal (DIP) joints.[7]
Two sesamoid bones are present at the first MCP joint. These are consistently present and have significant functional implications for the motion of the thumb. Single sesamoids appear over the second and fifth MCP joints in 60.8% and 59.1% of the population, respectively.[8]
Embryology
The limb bud first appears in the proximal fetus around the fifth week of development. From this point, various HOX genes govern the growth of the limb. The stylopod, zeugopod, and autopod are the three growth zones of the limb bud corresponding to the humerus, ulna and radius, and the hand, respectively. Ectoderm differentiates into the apical ectodermal ridge, nonridge ectoderm, and zone of polarizing activity. These zones carry essential roles in differentiation. For example, removal of the apical ectodermal ridge early in limb development will result in the presence of only stylopod development. Removal of the apical ectodermal ridge later in development will result in the development of the stylopod and zeugopod, but no autopod, leading to the fetus not developing a hand.[9]
The HOXA and HOXD genes are responsible for the embryologic development of the hand in humans. HOXA is responsible for anteroposterior growth, while HOXD is responsible for proximodistal growth.[10]
Research has demonstrated that the metacarpal bone length can contribute to the estimation of fetal development during the prenatal period, and this may help to evaluate any anomalies. Utilizing this in combination with foot lengths and other accepted estimates of development can provide a more comprehensive picture.[11]
Due to the complexity of the structure of the hand, a myriad of morphologic anomalies may occur during development.
Blood Supply and Lymphatics
Blood supply to the hand comes from ulnar and radial arteries, which are branches of the brachial artery. Dorsal hand vascular supply comes from the dorsal carpal arch. This arch forms from anastomosis of dorsal carpal branches of radial and ulnar arteries. Metacarpal branches subsequently arise from the dorsal carpal arch. The first metacarpal branch courses along the radial border of the second metacarpal, supplying the first web space and second metacarpal. The second through fifth branches course along the ulnar borders of the second through fifth metacarpals and provide branches to the interosseous muscles as well as the periosteum.[12]
Superficial palmar arterial arch is primarily formed by the ulnar artery, while the radial artery mainly supplies deep palmar arterial arch. Metacarpal branches generally arise from the deep arch, while digital arteries arise from the superficial arch. Metacarpal branches form anastomosis with digital arteries.[13]
Physiologic variation of arterial flow in the hand is plentiful with a multitude of anastomoses and variations in flow dominance.[14]
Nerves
Innervation to the hand is from the median, ulnar, and radial nerves.[15][16][17] Each digit/ray has two palmar and two dorsal digital nerves. The cutaneous volar aspect of the first three and a half digits is innervated by the median nerve. The ulnar nerve entirely innervates the dorsal and volar ulnar half of the fourth and the fifth digit. The radial nerve innervates the remainder of the dorsal hand. Due to the complex functionality of the hand, it is vital that clinicians reliably report and understand proprioception and grasp strength. A multiple innervation distribution is provided to the MCPs, PIPs, and DIPs to facilitate this understanding.[18]
Muscles
Three volar Interossei adduct the second, fourth, and fifth digits about an axis formed by the third digit. These muscles originate on the metacarpal of the digit being adducted and insert to their respective proximal phalangeal base and extensor hood. Adduction occurring along this third digit axis means that the volar interosseous muscle of the second digit is located on its ulnar border, while the interossei of fourth and fifth digit reside on their radial borders.[19]
Four dorsal interossei work to abduct the second, third, and fourth digits while assisting with flexion of the MCPs, extension of the PIPs, and extension of the DIPs. The first dorsal interosseous muscle originates from the first and second metacarpals, inserting to the radial base of proximal phalanx of the second digit as well as its extensor hood. The second dorsal interosseous muscle originates from second and third metacarpals, inserting to the radial base of proximal phalanx of the third digit as well as its extensor hood. The third dorsal interosseous muscle originates from third and fourth metacarpals, inserting to the ulnar base of proximal phalanx of the third digit as well as its extensor hood. The fourth dorsal interosseous muscle originates from fourth and fifth metacarpals, inserting to the ulnar base of proximal phalanx of the fourth digit as well as its extensor hood.[19]
Abductor pollicis longus (APL) originates in the forearm, at the midshaft of the radial border of ulna and the ulnar border of radius, as well as the interosseous membrane. It inserts to the radial side of the base of the first metacarpal in addition to the trapezium and opponens pollicis fascia.[20] This muscle acts to abduct the first digit.
Abductor pollicis brevis (APB) originates at trapezium and scaphoid and inserts to the lateral base of proximal phalanx of the first digit. This muscle acts in first digit abduction in addition to MCP flexion.[21]
Extensor pollicis longus (EPL) originates at the radial border of ulna and interosseous membrane, distal to the origin of APL. EPL inserts to the base of the distal phalanx and acts to extend the interphalangeal joint.[20]
Extensor pollicis brevis (EPB) originates at the ulnar border of the radius and interosseous membrane at the level of EPL. It inserts to the base of proximal phalanx of the first digit and aids in first digit extension at the MCP.[20]
Opponens pollicis acts to pronate the first metacarpal. It originates at trapezium and inserts to the anterolateral aspect of the first metacarpal.[21]
Flexor carpi radialis (FCR) originates at the medial humeral epicondyle and inserts to trapezium, second metacarpal, and third metacarpal. FCR acts to flex and radially deviate the wrist.[22]
Flexor pollicis brevis (FPB) has a deep and superficial head. Deep head originates at second metacarpal, while superficial head originates at transverse carpal ligament and trapezium. These insert to the lateral base of proximal phalanx of the first digit and act to flex the MCP.[21]
Flexor pollicis longus (FPL) is the primary flexor of the first digit, originating from the volar interosseous membrane and radius. It inserts to the base of the distal phalanx.[23]
Adductor pollicis has two heads, an oblique and transverse. The oblique head originates at the capitate, second, and third metacarpals. The transverse head originates at distal half of third metacarpal shaft. These both insert to the medial base of thumb proximal phalanx and act to adduct first digit.[21]
Abductor digiti minimi (ADM) acts to abduct the fifth digit and has been found to originate at the pisiform, piso-hamate ligament and flexor carpi ulnaris. It inserts to the ulnar aspect of proximal phalangeal base and extensor apparatus of the fifth digit.[24]
Flexor digiti minimi (FDM) originates from hamate, pisiform, and flexor retinaculum. Distally, it fuses with ADM to insert to the proximal phalangeal base of the fifth digit, leading to its action of MCP flexion.[24]
Extensor carpi ulnaris originates at the lateral humeral epicondyle and inserts to the dorsal base of the fifth metacarpal, acting in wrist extension and ulnar deviation.[25]
Flexor digitorum superficialis (FDS) has a broad origination from the medial epicondyle of humerus and coronoid process of the ulna to the volar aspect of the radial shaft. It then inserts to the middle phalangeal bases of second through fifth digits. This acts primarily in PIP flexion.[26]
Flexor digitorum profundus (FDP) originates from the volar-medial aspect of the ulna and interosseous membrane and inserts at the distal phalangeal bases of second through fifth digits. This performs DIP flexion.[27]
Extensor digitorum communis (central slip and terminal tendons) originates at the lateral epicondyle of humerus and inserts at the dorsal aspect of the distal phalangeal base of the second through fifth digits. There is significant anatomic variation in the accessory slips and insertions of this muscle, but the classic teaching is that there is an insertion to the middle phalanx and MCP in addition to this consistently present terminal insertion.[28]
Physiologic Variants
There is a great deal of physiologic variation between individuals in the morphology of the hand bones. One of the tools utilized to discuss the variance in hand anatomy is the digit length ratio of the second to the fourth digit, otherwise referred to as the 2D to 4D ratio. This number has demonstrated to be 0.98 among the general population but shows variability between ethnicities, races, and sexes, as well as the handedness of the patient. The third digit is consistently the longest of the digits. The most significant source of variance in the hand bones is the result of differences in size.[10]
Surgical Considerations
Metacarpal fractures should undergo fixation if there is any component of malrotation to ensure that patients can make a closed fist and grip properly.
Surgery is indicated in the treatment of these fractures when the fracture pattern falls outside of acceptable angulation tolerances, and thus the patient’s functional outcome would benefit from surgical fixation by lag screw fixation and/or plating techniques, or via percutaneous pinning of the fractures.[29][2] Tolerances for fractures of the shaft and neck of each metacarpal vary with the index tolerating the least angulation and the little finger tolerating the most. Fractures of the fifth metacarpal neck, otherwise known as boxer’s fractures highlight the good outcomes of nonoperative treatment of the majority of these fractures.[30][31]
include MCP or IP dislocations which are irreducible will also need to undergo surgical fixation to facilitate the restoration of function.[32] Phalanx fractures with displacement, nonunion, malunion, ipsilateral extremity fractures, pathologic fractures, or multiple unstable ipsilateral hand fractures may require surgical intervention.[33] Dorsal intraarticular fractures of the distal phalanx, otherwise known as mallet finger, rarely need to undergo surgical fixation, but intervention is indicated with greater than 30 percent involvement of the articular surface or for volar subluxation of the distal phalanx.[34] Volar interarticular avulsion fractures of the distal phalanx, also known as jersey finger, by in large require surgical fixation for the restoration of flexor digitorum profundus function.[35]
Clinical Significance
Polydactyly occurs once in every 700 to 1000 live births, making it a relatively common anatomical variant. There are a variety of types of polydactyly, and they can broadly categorize as syndromic or non-syndromic. Subtypes of polydactyly exist based upon the point of origination of the extra digit. Though the identities of the exact genetic links are still a work in progress, patients who present with polydactyly should have a careful workup to rule out underlying conditions.[36]
Small joint osteoarthritis characteristically demonstrates Heberden and Bouchard nodes of the DIP and PIP, respectively. These nodes represent the cutaneous manifestations of joint space narrowing and osteophyte formation resulting from osteoarthritis. Research shows a positive correlation between the appearance of these nodes and underlying osteoarthritis.[37]
Rheumatoid arthritis (RA) is another form of arthritis that often presents with prominent hand manifestations. Swan neck and boutonniere deformities are classically described, in addition to the ulnar deviation of the digits. The swan neck deformity is characterized by DIP flexion with PIP extension, while the inverse is true of the boutonniere deformity. Nowadays, disease-modifying antirheumatic drugs (DMARDs) have been able to reduce the severity of hand disease seen in RA, but early intervention should be started to prevent disability and progressive joint erosion seen in the natural course of the disease.[38]
(Click Image to Enlarge)
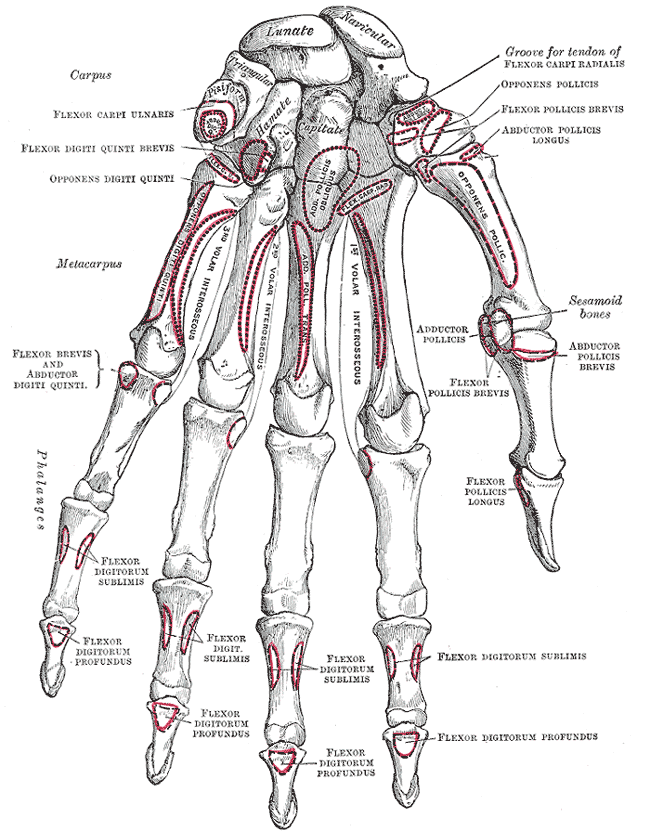
Volar, Left Hand, Carpus, Lunate, Navicular, Triangular, Pisiform, Hamate, Capitate, Flexor Carpi Ulnaris, Flexor digiti Quinti Brevis, Opponens Digiti Quinti, Metacarpus, Adductor pollicis, oblique head, Flexor carpus radialis, Abductor pollicis longus, Opponens pollicis, Flexor carpi radialis, Opponens Pollicis, Adductor pollicis, Sesamoid, Abductor pollicis brevis, Flexor Pollicis Brevis, Flexor carpi radialis, Adductor pollicis, obliques head, Opponens digiti minimi, Volar interosseous, Flexor Brevis, Abductor Digiti Quinti, Adductor Pollicis, Transverse head, Flexor pollicis longus, Flexor digitorum sublimis, Flexor digitorum sublimis, Flexor digitorum profundus, Phalanges, Hand, Surface,
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)

Right, Hand, Carpus, Metacarpus, Phalanges, Articulate with Radius, Navicular, Lunate, Pisiform, Triangular, Hamate, Capitate, Lesser multangular, Trapezoid, Greater multangular, Trapezium, Extensor Carpi radialis longus, Extensor carpi radialis brevis, Extensor Pollicis Brevis, Extensor Pollicis Longus, Extensor digitorum communis, Extensor indicis proprius, Dorsal Interosseous,
Contributed by Gray's Anatomy Plates
(Click Image to Enlarge)
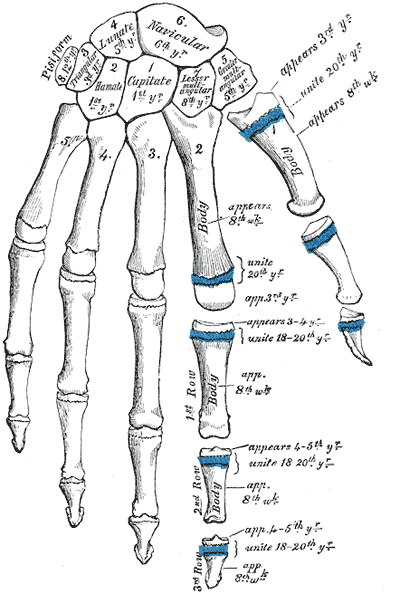
Development, Plan of, Hand, Pisiform, Triangular, Lunate, Navicular, Capitate, Hamate, Trapezoid, Trapezium, Phalanges, Metacarpals, Carpals
Contributed by Gray's Anatomy Plates