Dextrocardia
- Article Author:
- Raunak Nair
- Article Editor:
- Sujit Muthukuru
- Updated:
- 8/10/2020 10:54:24 PM
- For CME on this topic:
- Dextrocardia CME
- PubMed Link:
- Dextrocardia
Introduction
Dextrocardia is a rare congenital disorder in which the heart resides on the right side of the thoracic cavity. It is often associated with other development anomalies and, in most cases, is diagnosed incidentally. It can occur by itself or can be accompanied by a reversal in the position of other organs (termed situs inversus totalis).[1] Dextrocardia also involves a change in the orientation of the heart with its base to the apex axis being directed to the right, in contrast to the normal heart orientation where the apex is directed to the left. This change in orientation differentiates it from cardiac dextroposition, where the heart is displaced to the right side as a result of extracardiac causes, such as a diaphragmatic hernia, right pneumonectomy, or right lung hypoplasia.[2] In typical dextrocardia, the intracardiac anatomy is also reversed, termed as situs inversus. When dextrocardia is associated with a normal position of other thoracoabdominal structures, it is called situs solitus.[3]
Etiology
The exact etiology of dextrocardia is unknown. However, it is thought to be secondary to the abnormal position of the organs during embryonic development. Kartagener syndrome is an inherited disorder of ciliary motility that is caused by autosomal recessive mutation and is associated with chronic sinusitis, bronchiectasis, and dextrocardia.[4] Heterotaxy is another inherited condition that leads to malposition of internal organs and vessels and is caused by a lateralization defect during embryonic development.[5] Individuals with heterotaxy might also have other associated congenital disorders involving the abdominal organs, intestinal malrotation, systemic venous abnormalities, anomalous pulmonary venous connections, and asplenia.[6]
Epidemiology
Dextrocardia is a very rare condition, and studies have revealed incidence rates of dextrocardia to be around 1 in 12000 pregnancies.[7] Kartagener syndrome has an incidence rate of about 1 in 30,000 live births, and situs inversus totalis was seen in around 50% of patients with primary ciliary dyskinesia.[8] Isolated dextrocardia was seen in 0.6% of patients with primary ciliary dyskinesia.[9] There has been no ethnic or gender-related predilection described for dextrocardia.
Pathophysiology
Dextrocardia occurs as a result of abnormalities in the embryological development of the heart. The heart is the first organ to develop in an embryo. The fetal heart develops from an embryonic heart tube, which is formed by the fusion of the endocardial tubes. The heart tube attaches to the cranial aspect to the arterial trunk, and the caudal aspect is connected to the venous channels. Once the heart tube is formed, the next important step in the development of the heart is looping. Looping determines the position of the ventricle in relationship to the atria. The heart tube may loop to the right (termed as D loop) or loop to the left (termed as L-loop). With a D-loop, the morphologic right ventricle lies to the right of the left ventricle, whereas, with an L-loop, the morphologic right ventricle is positioned to the left of the left ventricle.[10][11][12] If a D-bulboventricular loop fails to migrate into the left hemithorax, it can result in dextrocardia with the heart in the right hemithorax. Similarly, if an L-bulboventricular loop completes the rotation in the right hemithorax, the heart can be situated in the right hemithorax. It is not entirely clear the circumstances leading to these aberrations in embryonic development; however, an association with a defect in dynein or ciliary motility has been implicated.[13]
History and Physical
Dextrocardia by itself (also termed as isolated dextrocardia) is asymptomatic, whereas dextrocardia with situs inversus and Kartagener syndrome can have a multitude of symptoms depending on the accompanying abnormalities. The history of these patients might reveal the following symptoms.[14][15][16]
- Cyanosis
- Dyspnea
- Failure to thrive
- Fatigue
- Jaundice
- Pallor
- Decreased exercise tolerance
- Repeated sinus or lung infections
- Hydrocephalus
- Arrhythmias, especially atrioventricular (AV) blocks
- Intestinal obstruction
The physical examination of a patient with dextrocardia might reveal cyanosis, clubbing, a prominent apical impulse on the right side of the chest, and easily audible heart sounds on the right side of the chest.
Evaluation
Dextrocardia is often diagnosed incidentally on the routine radiological examination, which reveals an abnormal location of the heart. Electrocardiogram (EKG) can also reveal the presence of dextrocardia as evidenced by right axis deviation, inversion of all complexes in lead I, upright p wave in AVL, and an absent R wave progression in the anterior leads.[17] Limb reversal might produce similar EKG findings; however, with a normal EKG pattern in the precordial leads. Echocardiogram, computed tomography (CT) scan of the chest, and magnetic resonance imaging (MRI) of the chest might all help evaluate for dextrocardia and associated anomalies.[18][19]
Nasal brush biopsy and nasal nitric oxide measurements are screening tests used to diagnose Kartagener syndrome.[20] CT scan of the chest might reveal bronchiectasis and dextrocardia in these patients. Genetic testing and electron microscopy are other available modalities to confirm the diagnosis of primary ciliary dyskinesia.
Treatment / Management
Most patients with dextrocardia are asymptomatic and lead a normal life.
The management of dextrocardia varies depending on the presence of other congenital anomalies. In patients who have other associated cardiac malformations such as defects of the walls of the heart, malposition of blood vessels, Tetralogy of Fallot, septal defects, severe valvular abnormalities, surgical reconstruction might need to be considered.[21][22]
- Patients with heart blocks and abnormalities of the cardiac electrical system need to be evaluated for pacemaker placement.[23]
- Although there is no cure for PCD available at the moment, management for these patients should involve mucolytics and expectorants to clear the secretions.
- Antibiotics might be required to fight off respiratory illness due to bacterial infections, especially in patients with accompanying asplenia.[24]
- In patients with severe bronchiectasis affecting the quality of life, lung resection surgery should be considered.[25]
- Neonates may present with intestinal obstruction requiring surgical management to prevent life-threatening complications.[26]
- Patients with dextrocardia and complex congenital heart malformations might require heart transplantation with the reconstruction of the venous pathways to accommodate a normal donor heart.[27]
Differential Diagnosis
The differential diagnosis for a heart located on the right side of the thoracic cavity is very narrow. However, dextrocardia must be differentiated from:
- Cardiac dextroposition: The heart is displaced to the right side as a result of extracardiac causes, such as a diaphragmatic hernia, right pneumonectomy, or right lung hypoplasia.
- Kartagener syndrome: Dextrocardia situs inversus is accompanied by primary ciliary dyskinesia.
- Dextroversion: The heart is abnormally positioned to the right and rotated.
- Transposition of the great vessels (TGA): The major vessels of the heart connect in reverse with a reversal of the heart chambers.
- Heterotaxy: Mirrored internal organs do not develop or function properly.
- Endocardial cushion defect
Prognosis
- The prognosis of patients with dextrocardia depends on the presence or absence of other accompanying congenital defects and the type of congenital anomalies.
- As mentioned before, patients with isolated dextrocardia have a normal lifespan without any complications.
- Newborns with dextrocardia and asplenia are easily susceptible to bacterial infections (especially infections from encapsulated organisms such as Streptococcus pneumoniae, Haemophilus influenzae, and Meningococcus) and life-threatening bacteremia. These patients might need to be on antibiotic prophylaxis.
Complications
- Failure to thrive
- Respiratory failure
- Congestive heart failure
- Severe infections, especially from encapsulated organisms.
- Infertility in males in Kartagener syndrome
- Recurrent sinusitis and pneumonia
- Intestinal obstruction due to malrotation
Consultations
Genetic counseling may be helpful for patients and their affected families to understand more about the disease and its associated conditions.
Deterrence and Patient Education
Dextrocardia is a clinical condition characterized by the location of the heart on the right side of the chest cavity. Though isolated dextrocardia is a benign condition, it can often be associated with other congenital anomalies, which can lead to several problems such as failure to thrive, recurrent infections, and breathing difficulties in newborn and neonates. Adults with dextrocardia might also have accompanying infertility. Upon suspicion, a thorough evaluation that involves imaging and genetic analysis is necessary to assess for other accompanying abnormalities.
Enhancing Healthcare Team Outcomes
Though not a common occurrence, an understanding of the incidence, presentation, etiology, and management of dextrocardia are essential for all providers, identification of this disorder might be pivotal to recognize rare presentations of Kartagener syndrome or heterotaxy. Due to the possibility of other congenital anomalies associated with dextrocardia, diagnosing dextrocardia could be a bridge to the diagnosis of other cardiac anomalies. Due to the advances in medicine, patients with complex congenital heart disease often live a long healthy life. Understanding the pathophysiology behind this condition is important for anesthetic considerations when these patients undergo cardiac or non-cardiac surgery. Thus, awareness and knowledge about dextrocardia and its implications are vital in improving the care provided to patients.
Patients with dextrocardia benefit from care by an interprofessional team consisting of primary care, radiologists, cardiologists, cardiothoracic surgeons, and infections disease specialists. [Level 5]
(Click Image to Enlarge)

dextrocardia chest x-ray
Image courtesy S Bhimji MD
(Click Image to Enlarge)
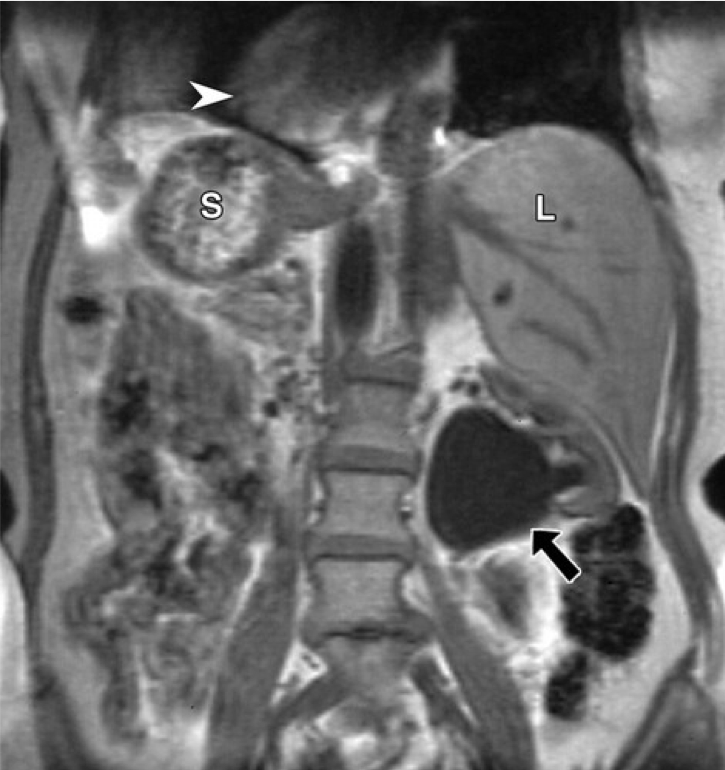
Situs inversus in a 56-year-old woman with left flank pain. Coronal unenhanced fat-suppressed T1-weighted MR image of the abdomen reveals a left ureteropelvic junction obstruction (arrow). The liver (L) is located in the left upper quadrant, and the stomach (S) and spleen (not shown) are located in the right upper quadrant. Dextrocardia (arrowhead) is also noted.
Contributed from Abdominal Manifestations of Situs Anomalies in Adults by Ann S. Fulcher, Mary Ann Turner (https://pubs.rsna.org/doi/full/10.1148/rg.226025016) [free access]