Anatomy, Thorax, Triangle of Auscultation
- Article Author:
- Nazish Malik
- Article Author:
- Brandon Tedder
- Article Editor:
- Michael Zemaitis
- Updated:
- 8/22/2020 7:39:52 PM
- For CME on this topic:
- Anatomy, Thorax, Triangle of Auscultation CME
- PubMed Link:
- Anatomy, Thorax, Triangle of Auscultation
Introduction
When assessing a patient clinically, it is important to know basic anatomical details which will aid the clinician during the physical examination. Assessment of the thorax is a fundamental part of any physical examination as the location of many vital structures are in this region. On the dorsum of the thorax, there exists a relative thinning of the muscles that provide an essential anatomical landmark which aids clinicians during pulmonary auscultation and various thoracic procedures – the triangle of auscultation.
Structure and Function
The triangle of auscultation is at the inferior angle of the scapula best exposed by instructing the patient to cross his arms over his chest and bending forward. It is bordered on three sides – inferiorly by the latissimus dorsi muscle, superiorly by the inferior border of the trapezius, and laterally by the medial border of the scapula formed by the teres major muscle and infraspinatus muscle.[1] The floor of the triangle consists of the posterior thoracic wall which contains the rhomboid major muscle, serratus anterior muscle, and erector spinae muscles.
The triangle of auscultation is an important anatomical landmark that allows for better auscultation during the pulmonary examination.[2] When the patient crosses their arms across their chest, the scapula and muscular borders of the triangle of auscultation move in a way to expose the landmark. As a result, there are fewer impedances between the examiner’s stethoscope and the lungs which allow for better auscultation.[3] As a result, auscultation of breath sounds such as wheezing, rhonchi, and rales of the inferior lobes of the lungs is optimal in this area.
Embryology
Skeletal muscle formation occurs through the process of myogenesis.[4] These cells originate from the para-axial mesoderm which forms somites. They then arrange to form the dermatomyotome and finally arrange to form the myotome. Skeletal muscle ultimately forms in three stages the myoblast stage, myotubule stage, and the myofiber stage. The myoblasts are the progenitor cells of skeletal muscle and coalesce to form giant multinucleated cells. They then create myofibers on which the structural framework builds. The muscle cells respond to fibroblast growth factor and release extracellular matrix proteins which ultimately form the myotubules. The myoblast continues to fuse and proliferate in a linear sequence.[5] The myotubules fuse to form larger myofibers and as fibroblast growth factor supplies diminish the cells stop dividing leading to quiescent multinucleated giant cells. However, there remain myosattelite cells along the basement membrane which are the precursors to skeletal muscle. They can proliferate into additional muscle tissue or provide myonuclei upon activation.[6][7]
Blood Supply and Lymphatics
The thoracic wall receives vascular supply from branches of the subclavian artery and the thoracic aorta. These larger vessels give off smaller tributaries such as the internal thoracic arteries, posterior intercostal, and subcostal arteries. The latissimus dorsi muscle gets its supply from the thoracodorsal artery, the trapezius by the transverse muscular branches, the teres major by the subscapular and circumflex scapular arteries, and the infraspinatus by the suprascapular and circumflex scapular arteries. Inside the thorax lies the heart, the ascending thoracic aorta, the aortic arch, and its branches, and the descending thoracic aorta; this is important relative to performing resuscitative thoracotomies in response to severe thoracic or abdominal trauma where the patient has entered into some form of cardiac arrest. Clinicians can control thoracic hemorrhage, relieve tamponade, and repair injuries to underlying organs.[8]
Muscles
Lattisimus Dorsi
The latissimus dorsi is a large muscle forming the inferior border of the triangle of auscultation. It originates from the spinous processes of thoracic vertebrae seven though lumbar vertebrae five, the thoracolumbar fascia, the inferior angle of the scapula, the lower ribs, and iliac crest of the sacrum. It inserts onto the floor of the bicipital/intertubercular groove of the humerus. It acts to adduct, medially rotate, and extend the arm at the glenohumeral joint. It is innervated by the thoracodorsal nerve which originates from nerve roots C6 to C8.
Trapezius
The inferior border of the trapezius muscle forms the superior border of the triangle of auscultation. The trapezius muscle originates from the spinous process of cervical vertebrae seven through thoracic vertebrae 12. It also originates from the protuberance of the occipital bone, ligamentum nuchae, and medial superior nuchal line. It inserts onto the lateral clavicle, the spine of scapula, and the acromion. There are three divisions of the trapezius muscle: the upper fibers, middle fibers, and lower fibers (the inferior border of the trapezius). The upper fibers act to elevate and superiorly rotate the scapula and extend the neck. The middle fibers function to adduct the scapula. The lower fibers serve to stabilize the scapula even further and assist the upper fibers in rotation of the scapula. Motor function of the trapezius derives from the accessory nerve, and proprioception follows the ventral rami of C3 and C4.
Teres Major
The teres major muscle forms the medial border of the triangle of auscultation along with the infraspinatus muscle. The teres major muscle originates from the inferior angle and lateral border of the scapula and inserts onto the intertubercular groove of the humerus. It acts to adduct, medially rotate, and extend the arm at the glenohumeral joint. It is innervated by the lower scapular nerve which originates from nerve roots C5 to C7.
Infraspinatus
The infraspinatus muscle along with the teres major muscle forms the medial border of the triangle of auscultation. The infraspinatus muscle originates from the infraspinous fossa of the scapula and inserts onto the greater tubercle of the humerus. It acts to laterally rotate the glenohumeral joint and helps stabilize the shoulder. It is innervated by the suprascapular nerve which consists of nerve roots C5 through C6.
Surgical Considerations
A thoracotomy is a procedure in which the thorax is opened surgically to gain access to the internal structures such as the lungs, pulmonary vasculature, heart, or aorta. This procedure is sometimes necessary to emergently evacuate a pericardial tamponade, control thoracic hemorrhage, internal cardiac massage or cross-clamp the descending thoracic aorta. Access through the triangle of auscultation provides the patient with less perioperative morbidity as it spares incision through the latissimus dorsi.[9] Additionally, a pleurectomy is another procedure performed through thoracotomy access through the triangle of auscultation; this is useful in patients who have recurrent spontaneous pneumothoraces, as artificial obliteration of the pleural space and closure through a formal thoracotomy lead to excessive pain and discomfort.[10][11]
Clinical Significance
As stated above, the triangle of auscultation is an important anatomical landmark which allows for prime pulmonary auscultation. Auscultation of breath sounds is part of performing a routine lung examination. If a clinician does not hear equal air entry bilaterally, then it is time to consider conditions leading to airway obstruction such as inhaled foreign objects or a collapsed lung. If auscultation reveals wheezes, then the patient could have an obstructive condition such as chronic obstructive pulmonary disease (COPD) or asthma. If rhonchi are heard then the patient could be suffering from COPD, bronchiectasis, pneumonia, bronchitis, or cystic fibrosis. If the examiner hears rales, then fluid is trapped inside the alveoli and could be secondary to heart failure or pulmonary infection. An examiner can encounter all these findings during the pulmonary examination. The triangle of auscultation allows the clinician to listen better to the patient's lungs and guide them to the proper diagnosis.
(Click Image to Enlarge)
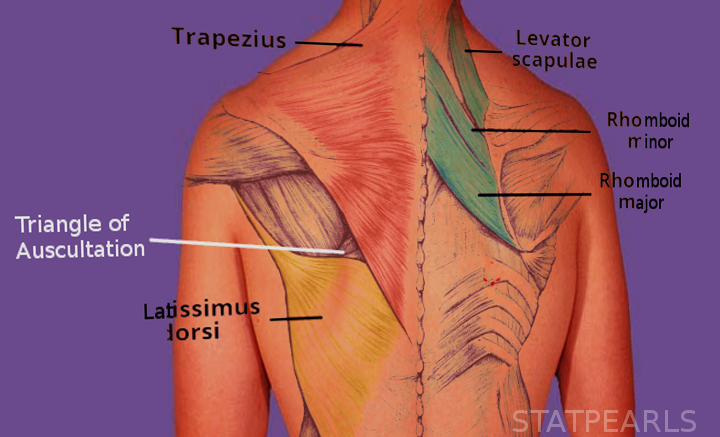
Triangle of Auscultation
Image courtesy S Bhimji MD