Anatomy, Shoulder and Upper Limb, Elbow Annular Ligament
- Article Author:
- Brian Fliegel
- Article Author:
- John Ekblad
- Article Editor:
- Matthew Varacallo
- Updated:
- 7/31/2020 3:17:26 PM
- For CME on this topic:
- Anatomy, Shoulder and Upper Limb, Elbow Annular Ligament CME
- PubMed Link:
- Anatomy, Shoulder and Upper Limb, Elbow Annular Ligament
Introduction
The annular ligament is located within the elbow joint. The elbow joint is comprised of three bones that form three articulations which are all contained within the elbow joint capsule. The humerus, radius, and ulna interact in a complex, dynamic relationship to constitute three distinct joint articulations:[1]
- Ulnohumeral articulation
- Distal humerus (trochlea) and the proximal ulna (trochlear notch, or greater sigmoid notch)
- Radiocapitellar articulation
- Distal humerus (capitellum) and the proximal radius (radial head)
- Proximal radioulnar articulation
- The proximal ulna (radial notch, or lesser sigmoid notch) and the proximal radius (radial head)
The elbow joint is both a uniaxial, hinge joint (ulnohumeral articulation) and a pivot joint (radiocapitellar articulation). The ligaments surrounding the elbow joint connect one bone to another and provide static stability while allowing the motion to occur. The annular ligament is a critical component of the lateral collateral ligament (LCL) complex. While the major roles of the ulnar collateral ligament (UCL) and the LCL complex include primary support against excessive valgus stress and varus stress, respectively, the annular ligament plays an additionally important role as a primary stabilizing structure for the radial head articulation with the radial notch of the proximal ulna during forearm supination and pronation.[1]
Structure and Function
The annular ligament is a strong fibro-osseous circular structure that has attachments to the anterior and posterior margins of the radial notch (lesser sigmoid cavity) of the ulna. The annular ligament forms about four-fifths of a circle. The ligament subdivides into three layers:[2]
- Deep capsular structure
- Intermediate layer (annular ligament proper)
- Superficial structure
The annular ligament proper is composed of a superior oblique band and an inferior oblique.[3] Superiorly, the annular ligament is at its widest diameter and is continuous with the fibrous capsule of the elbow joint. Inferiorly, the ligament tapers as it surrounds the head and neck of the radius demonstrating distinct attachment sites to the radial neck via a synovial membrane; this allows the radius to freely rotate during forearm pronation and supination while preventing distal displacement. The anterior portion and posterior portions of the annular ligament become maximally taut when the forearm is in terminal supination and pronation, respectively.[4]
Lateral collateral ligament (LCL) complex of the Elbow
Four ligaments form the LCL complex of the elbow. These ligaments include the annular ligament, accessory collateral ligament, lateral ulnar collateral ligament, and the radial collateral ligament. The LCL complex originates on the lateral humeral epicondyle.[5]
While the annular ligament plays a static stabilizing role against excessive varus stress at the elbow, the annular ligament's primary stabilizing role functions at the proximal radioulnar articulation. The annular ligament stabilizes the radial head within the radial notch of the ulna as it rotates during supination and pronation of the forearm.
The proximal, central, and distal band of the interosseous membrane also assists in proximal radial head stabilization. Under transverse displacement, the annular ligament along with the central and proximal band of the interosseous membrane equally contribute to stabilizing the radius. However, during forearm pronation and supination, the central band of the interosseous membrane contributes more to the stabilization of the radial head than the annular ligament and proximal band.[6]
Embryology
The annular ligament is a musculoskeletal structure and like the other ligaments throughout the body is derived from mesenchymal cells. The synovial membrane lining the space between the radial head and the annular ligament is also derived from mesenchymal cells. The annular ligament develops as a densification of the elbow joint capsule and becomes defined by week 12.[7] By week 22 the annular ligament is well developed.[8]
Blood Supply and Lymphatics
The blood supply to the elbow joint derives from peri-articular anastomoses. Collateral and recurrent arterial branches from the brachial, deep brachial, ulnar, and radial arteries anastomose to provide consistent blood flow. The superior collateral branches include the radial collateral artery, superior ulnar collateral artery, and inferior ulnar collateral artery. The inferior collateral branches include the anterior ulnar recurrent artery, posterior ulnar recurrent artery, the radial recurrent artery, and the recurrent interosseous artery. The radial, ulnar, basilic, and brachial veins provide the elbow joint's venous outflow system.[9]
There are two different sets of lymph nodes at the elbow, the superficial and deep cubital nodes. They are above the medial epicondyle. The superficial cubital nodes drain the medial side of the hand and the forearm. The deep cubital nodes drain the elbow joint itself. The efferent vessels travel more proximal and drain into the axillary lymph nodes before entering the thoracic duct on the left side and the right lymphatic duct on the right side.
Nerves
Anteriorly, the elbow joint is innervated by branches of the median, radial, and musculocutaneous nerves. Posteriorly, the elbow joint receives innervation by branches of the ulnar nerve. The anterolateral aspect of the elbow capsule is innervated by branches of the radial nerve which is where the annular ligament is located.[10]
Muscles
The muscles crossing the elbow joint are subdivided into the flexors and extensors.
The primary elbow flexors include the biceps brachii and brachialis muscles. The biceps brachii is the largest of the flexors, and its primary function is as a primary and powerful forearm supinator.[11] The brachialis originates off the anterior humerus and inserts at the tuberosity of the ulna.[12] Additional elbow flexion occurs via the brachioradialis and pronator teres muscles. The brachioradialis originates from the lateral supracondylar humerus and attaches at the lateral aspect of the distal radius and assists in elbow flexion.[13] The pronator teres originates off the medial epicondyle of the distal humerus, as well as the coronoid, before inserting on the mid-lateral radial shaft. These attachments allow the pronator teres to assist in elbow flexion and forearm pronation.[14]
The extensors include the triceps brachii and anconeus. The triceps brachii is the largest extensor of the elbow and stabilizes the joint when the hand undergoes fine motor movements.[15] The anconeus is a small muscle that assists in elbow extension as well.[16]
Physiologic Variants
The annular ligament can demonstrate significant anatomic variation in its overall morphology. Multiple MRI-based studies and cadaveric dissection reports demonstrate the annular ligament appearing as a bi-lobed structure. Other studies demonstrate a morphologically broad annular ligamentous structure spanning superior to inferiorly at its attachment sites. In the instances that the ligament is bilobed, the anterior component remains its own separate, single band, while the posterior component demonstrates a fenestrated morphology. The latter can be seen as its own superior and inferior subdivisions, creating a funnel-shaped appearance.[17]
There are many variants of the synovial fold of the annular ligament. Not all people have a synovial fold. The synovial fold is its own distinct structure attached to the proximal end of the annular ligament, extending into the radiocapitellar joint capsule and blending with the common extensor tendon; this forms a single enthesis at the lateral epicondyle. The synovial fold can appear “meniscus-like” but is not a true meniscus. This fold can vary in thickness and can be an underlying cause of chronic, recalcitrant elbow pain syndromes.[18]
Surgical Considerations
Although many injuries involving the annular ligament can be managed conservatively with physical therapy, activity modifications, bracing, and non-steroidal anti-inflammatory medications (NSAIDs), there are many indications for surgical intervention.
Radial head instability
Healthcare providers must recognize that, in general, isolated radial head instability is extremely uncommon.[19] In effect, this finding is almost always seen as a long-standing congenital condition or in association with additional forearm trauma (i.e., Monteggia fracture patterns). The latter is extremely important to recognize clinically, as management is nearly always observation alone.[20]
Patients with congenital radial head dislocations will present with a separate chief complaint, and the dislocation may be discovered incidentally. These patients may be asymptomatic, and the following factors support congenital dislocation over an acute, traumatic dislocation:[8][21]
- Bilateral radial head dislocations
- Hypoplastic capitellum and convex radial head
- Other congenital abnormalities
- No history of trauma
- Inability to reduce
There have been case reports of a portion of the annular ligament band interposing between the humeroradial interface as the band slips over the radial head during elbow flexion and extension. This "snapping" or "locking" can be thought of as analogous to a bucket handle tear of the meniscus in the knee. Patients are managed based on the severity of symptoms and the degree of disability that is attributable to these mechanical symptoms. Persistent mechanical symptoms may warrant surgery to remove the interposed fragment.[22]
Annular ligament reconstruction techniques
The annular ligament is typically reconstructed using any of the following techniques.
- Bell-Tawse technique[23][24][24]
- Utilizes the central portion of the triceps tendon to create a strip of tissue to pass around the radial neck and through a single drill hole in the ulna
- Modifications of the original technique have included either an additional ulnar shortening osteotomy or in using the lateral portion of the triceps tendon with a transcapitellar pin for stability
- Two-hole technique[25]
- Seel and Peterson drilled two holes in the proximal ulna at the original sites of the normal attachment of the annular ligament
- A third technique was described utilizing small bone staples and bone-anchoring devices as an alternative to transosseous drill holes[19]
Rehabilitation protocols depend on the specific surgical technique used for the reconstruction and follow surgeon preference. General rehabilitation phases include early range of motion to mitigate the risks of postoperative stiffness. Patients should return to full range-of-motion by 6 weeks after surgery. Strengthening exercises begin at about 8 to 12 weeks postop. Most patients can return to normal activities by six months to one year. Overhead athletes may take over a year to return to sport.
Clinical Significance
An annular ligament injury is much more common in children due to the skeletal immaturity of the elbow joint during development. Three common injuries associated with the annular ligament are radial head or neck fractures, nursemaid elbow dislocations, and Monteggia fracture patterns.[26]
A radial head or neck fracture occurs during a fall on an outstretched hand or trauma/falls with the elbow in extension and forearm in pronation. Because the annular ligament wraps around the head of the radius, a fracture in this area can lead to damage to the ligament, and could potentially compromise joint stability as a sequela of the original injury.[27]
In pediatric patients, a radial head subluxation, also known as a nursemaid elbow or a pulled elbow, occurs due to a sudden pull on an extended arm, often when a parent lifts a child by the wrist or a fall.[28] This injury occurs almost entirely in the pediatric population since the annular ligament has increased laxity in children compared to adults. The average age is 1-4 years old and girls are more susceptible than boys. Children above the 75th percentile for weight are more frequently affected by this condition.[29] The classic symptoms of a radial head subluxation in pediatric patients consists of a history of the child refusing to use the arm. The child may hold the extremity with the elbow in extension with the forearm pronated or slightly flexed with the forearm pronated. On exam, there is typically pain localized to the dorsal aspect of the proximal forearm with typically no swelling.[30] Often there may only be subtle decreases in flexion and extension range of motion, but supination is significantly limited. The annular ligament is frequently interposed between the radial head and the capitellum of the humerus. X-ray of the elbow is usually unnecessary since the diagnosis can be made clinically, although after two failed attempts to reduce the dislocation imaging should be considered.[30] Treatment includes closed reduction using either hyperpronation or a combination of flexion and supination maneuvers. The prognosis in these patients is typically excellent in the long-term.[31]
Monteggia fracture-dislocations are relatively rare injuries in the pediatric population. Although forearm fractures are the most common fracture in the pediatric population, Monteggia fracture-dislocations constitute only about 1% of all pediatric forearm fractures.[32][33][32] These injuries have a proximal one-third of the ulna (olecranon) fracture with an associated radial head dislocation from the annular ligament. Mechanisms of injury include a fall on an outstretched hand with excessive forearm pronation and less commonly, direct trauma on the dorsal surface of the proximal forearm. These injuries commonly require surgical intervention given the high incidence of long-term elbow dysfunction following either missed injury or following suboptimal clinical management.[34] Surgical management consists of open reduction internal fixation of the proximal ulna. Upon restoration of ulnar length and stability, the radial head can be reduced with a restoration of the anatomic relationship between the radial head, capitellum, and the annular ligament.[35]
The prognosis in children with Monteggia fractures is usually good with early intervention and treatment. However, several studies in the literature have focused on the long-term clinical and radiographic outcomes following surgical management of pediatric patients with delayed/missed diagnosis of Monteggia fracture-dislocations. The most commonly performed procedure includes an open reduction with ulnar osteotomy with or without annular ligament reconstruction.[36]Nakamura et al. reported good long-term outcomes when performing open reduction if the patient is less than twelve years of age or within three years after the initial injury.[37]
(Click Image to Enlarge)
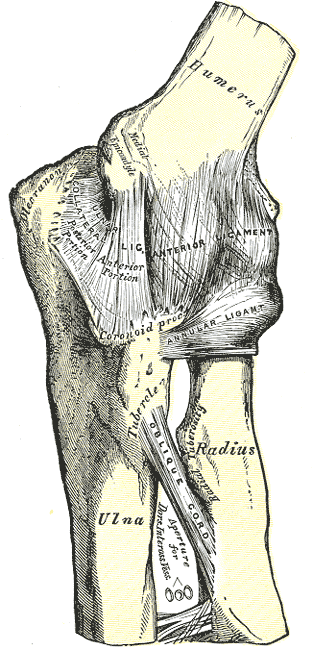
Elbow, Joint, Humerus, Internal Ligament, Olecranon, Ulnar Collateral Ligament, Anterior Ligament, Coranoid Process, Annular Ligament, Tubercle, Radius, Ulna, Oblique Cord
Contributed by Gray's Anatomy Plates