Anatomy, Bony Pelvis and Lower Limb, Femoral Muscles
- Article Author:
- Alyssa Ransom
- Article Author:
- Margaret Sinkler
- Article Editor:
- Shivajee Nallamothu
- Updated:
- 10/30/2020 8:20:58 AM
- For CME on this topic:
- Anatomy, Bony Pelvis and Lower Limb, Femoral Muscles CME
- PubMed Link:
- Anatomy, Bony Pelvis and Lower Limb, Femoral Muscles
Introduction
The muscles of the femoral region of the lower limb are divided into three compartments. The anterior or extensor, medial or adductor, and posterior or flexor compartments. Each compartment is separated from the others by an intermuscular septum that runs from the fascia lata to the linea aspera of the femur. The anterior compartment includes pectineus, iliopsoas, psoas minor, iliacus, sartorius and the quadriceps muscles. These muscles arise from the hip, spine, and proximal femur. The medial compartment is made up of the adductor magnus, adductor longus, adductor brevis, gracilis and obturator externus. These muscles originate near the anteroinferior external surface of the bony pelvis and insert at the linea aspera. The posterior compartment is made up of a group of muscles called the hamstrings, including semitendinosus, semimembranosus and biceps femoris. These muscles arise from the ischial tuberosity and the femur and insert on the medial tibia and lateral fibula. [1][2][3]
Structure and Function
The three compartments of the femoral region each have a distinct function. The anterior or extensor compartment is responsible for flexion of the hip and extension of the knee. The posterior or flexor compartment are the prime extensors of the hip and flexors of the knee. The medial or adductor compartment is composed of the adductors of the thigh.[4][5]
Fascial compartments separate the muscles of the thigh in order to create the compartments outlined above. The intermuscular septae are extensions of the fascia lata and attach to the linea aspera of the femur. The lateral intermuscular septum separates the anterior and posterior compartments. The medial intermuscular septum separates the anterior and medial compartments. The posterior intermuscular septum separates the medial and posterior compartments.
The fascia lata is deep fascia surrounding the thigh. This fascia layer acts to limit the outward expansion of the thigh muscles. The iliotibial (IT) tract is a thickened portion of the fascia that is found on the lateral aspect of the thigh. The aponeurosis of the tensor fasciae latae and gluteus maximus muscles also contribute to the IT tract. Inferior to the inguinal ligament, the saphenous opening allows for the passage of the great saphenous vein.
Anterior Compartment
The pectineus adducts, flexes, and assists in medial rotation of the thigh. The pectineus is a small square muscle that is found in the superomedial area of the thigh. Originating from the superior pubic ramus and inserting on the pectineal line of the femur. [6][7][8]
The iliopsoas is made up of the psoas major and minor, and the iliacus. These muscles work together to flex the hip joint as well as stabilize this joint during standing. The psoas major originates from the transverse processes of the T12 to L5 vertebrae. The psoas major then passes down through the pelvis and under the inguinal ligament to insert of the lesser trochanter of the femur. The psoas minor, found anterior to the psoas major, originates from the T12 through L1 vertebrae and then inserts on the pectineal line. The iliacus originates from the iliac crest, iliac fossa, ala of the sacrum, and anterior sacroiliac ligaments. It joins the psoas muscles traveling deep to the inguinal ligament and inserts on the tendon of the psoas major and the distal part of the lesser trochanter of the femur.
The sartorius flexes, abducts, and laterally rotates the thigh at the hip joint. It also aids in the flexion of the knee joint and the medial rotation of the leg in this position. The sartorius is a long band-like muscle that runs lateral to medial crossing the anterior aspect of the thigh. It originates from the anterior superior iliac spine and runs superficially to the quadriceps muscles and inserts on the superomedial surface of the tibia via the pes anserinus. It is the longest muscle in the body.
The quadriceps include four large muscles, rectus femoris, vastus lateralis, vastus medialis and vastus intermedius. The quadriceps femoris is one of the strongest muscle groups in the body that covers the anterior aspect of the femur. This group of muscles has a common function. They extend the leg at the knee joint. The rectus femoris has an additional role in stabilizing the hip joint and aiding in the flexion of the thigh. The rectus femoris originates from the anterior inferior iliac spine. It is named for its course straight down the anterior part of the thigh. The vastus lateralis is the largest muscle in the quadriceps. The vastus lateralis originates from the greater trochanter and is found on the lateral aspect of the thigh. The vastus medialis originates from the intertrochanteric line and medial lip of the linea aspera of the femur. It covers the medial aspect of the femur. Vastus intermedius originates from the anterior and lateral shaft of the femur. It can be found lying between the vastus lateral is and the vastus medialis, just deep to the rectus femoris. The quadriceps tendon is a common tendon for all four quadriceps muscles, which inserts into the patella. The patellar ligament extends from the patella to the tibial tuberosity.
Posterior Compartment
The hamstring consists of a group of 3 muscles.
The semitendinosus extends the hip and flexes the knee. The muscles originates at the ischial tuberosity and inserts at the medial surface of the tibial via a structure called the pes anserinus.
The semimembranosus extends the thigh, flexs the leg, and medially rotates the leg when the knee is flexed. The muscle originates on the ischial tuberosity and inserts on the medial condyle of the tibia.
The biceps femoris flexes the leg and when the knee is flexed rotates it laterally, and aids in the extension of the thigh. The biceps femoris has a long and short head. The long head originates on the ischial tuberosity and inserts on the head of the fibula. This head receives innervation from the tibial portion of the sciatic nerve. The short head of the biceps femoris originates on the linea aspera of the femur and inserts on the head of the fibula. This head receives innervations from the fibular portion of the sciatic nerve.
Medial Compartment
The adductor longus is a major adductor of the thigh. The muscle is the most anterior muscle in the group. It fans out from its origin on the anterior aspect of the pubis and inserts on the linea aspera of the femur. It covers both the anterior portion of the adductor brevis and the central portion of the adductor magnus.
The adductor brevis aids in adduction of the thigh and to a smaller extent flexion. The adductor brevis is the smallest of the group, lying just deep to pectineus and adductor longus. It originates from the body and inferior ramus of the pubis and inserts on the proximal portion of the linea aspera. This muscle divides the obturator nerve into an anterior and posterior division.
The adductor magnus contains both an adductor part and a hamstring part. The adductor part adducts and flexes the thigh. The hamstring part extends and adducts the thigh. The adductor magnus is the largest of the adductor muscles and is the most posterior of the adductor muscles, which crosses into the posterior compartment. The adductor portion originates from the inferior ramus of the pubis and inserts on the linea aspera and the medial supracondylar ridge. This portion of the muscle has an opening in the tendon allowing for the passage of important vessels to the posterior side of the knee. The hamstring portion originates from the ischial tuberosity and inserts of the adductor tubercle of the femur.
The gracilis adducts the thigh, flexes the leg, and aids in medial rotation of the leg. The gracilis is the weakest and most medial of the adductor muscles. It can be recognized by its long slender appearance. It crosses both the hip and the knee joint, originating from the body and inferior pubic rami and inserts with two other muscles in the pes anserinus which attaches to the medial surface of the tibia.
The obturator externus is a lateral rotator of the thigh and is a major stabilizer of the head of the femur in the acetabulum. The obturator externus is a small muscle found in the superomedial area of the thigh. The muscle originates from the external surface of the obturator membrane and inserts on the posterior side of the greater trochanter. It passes distally to the neck of the femur and the acetabulum.
Embryology
The lower limb bud appears during the fifth week of development, growing laterally from the L2 through S2 segments. Each limb bud contains the 3 primary germ layers: ectoderm, endoderm, and mesoderm. The lateral plate somatic mesoderm gives rise to skeletal elements, and the musculature arises from the myotomic portions of somites. The lower limb rotates 90 degrees medially along the longitudinal axis; allowing the knee to face anteriorly. Programmed apoptosis occurs in order to form the digits.
Blood Supply and Lymphatics
The anterior compartment of the thigh receives blood from the femoral artery, which comes from the external iliac. The femoral artery travels laterally to the femoral vein down the anterior thigh then passes to the posterior thigh through the adductor hiatus. The deep artery of the thigh is the largest branch of the femoral artery. It dives deep and passes posteriorly to the adductor longus to supply the adductor magnus, hamstrings, and vastus lateralis. The medial and lateral circumflex femoral arteries branch off the deep artery of the thigh and run around the head of the femur to supply the muscles in that area. The obturator artery splits into anterior and posterior branches and helps supply the adductor muscles.
The lymph from the leg travels to the superficial popliteal lymph nodes. The lymph vessels travel along with the femoral vessels to the deep inguinal lymph nodes. Lymph from the superficial tissues if the thigh drain to the superficial inguinal nodes. These drain to the external and common iliac the right and left lumbar lymph nodes. These then drain to the cisterna chyli and then the thoracic duct.
Nerves
The all of the anterior compartment of the thigh is innervated by the femoral nerve with the exception of the psoas major and minor, which are innervated by the anterior rami of the lumbar nerves (L1, L2, L3). The femoral nerve (L2, L3, L4) runs from the abdomen under the inguinal ligament to enter the later side of the femoral triangle. The nerve then divides into several branches. The medial compartment of the thigh is innervated by the obturator nerve (L2, L3, L4). The only exception to this is the hamstring portion of the adductor magnus which is innervated by the tibial part of the sciatic nerve (L4). The posterior compartment of the thigh is innervated by the sciatic nerve that is made up of a tibial and fibular division. The semitendinosus and semimembranosus are innervated by the tibial division of the sciatic nerve (L5, S1, S2). Biceps femoris has dual innervation; the long head is innervated by the tibial nerve and the short head by the fibular division of the sciatic nerve (L5, S1, S2).
Muscles
Anterior Thigh Muscles
Pectineus
- Origin: superior ramus of pubis
- Insertion: pectineal line of femur
- Action: adduction and flexion of thigh
- Innervation: femoral nerve (L2-4)
Iliopsoas (Illiacus + Psoas)
- Origin: T12-L5 vertebrae and ilium
- Insertion: lesser trochanter of femur
- Action: flexion of hip and hip stabilization
- Innervation: femoral nerve, psoas receives innervation from anterior rami L1-3
Sartorius
- Origin: anterior superior iliac spine
- Insertion: medial aspect of tibia via pes anserinus
- Action: flexion, abduction, and lateral rotation of hip; flexion of the knee
- Innervation: femoral nerve
Quadriceps Femoris (4 muscles)
Rectus femoris
- Origin: anterior inferior iliac spine
- Insertion: patella via quadriceps tendon
- Action: extension of the knee
- Innervation: femoral nerve
Vastus lateralis
- Origin: greater trochanter and linea aspera
- Insertion: patella via quadriceps tendon
- Action: extension of the knee
- Innervation: femoral nerve
Vastus medialis
- Origin: intertrochanteric line and linea aspera
- Insertion: patella via quadriceps tendon
- Action: extension of the knee
- Innervation: femoral nerve
Vastus intermedius
- Origin: femur shaft
- Insertion: patella via quadriceps tendon
- Action: extension of the knee
- Innervation: femoral nerve
Posterior Thigh Muscles
Semitendinosus
- Origin: ischial tuberosity
- Insertion: medial tibial surface via pes anserinus
- Action: extension of the hip, flexion of the knee
- Innervation: sciatic nerve (tibial portion, L4-S3)
Semimembranosus
- Origin: ischial tuberosity
- Insertion: medial condyle of tibia
- Action: extension of the hip, flexion of the knee
- Innervation: sciatic nerve (tibial portion, L4-S3)
Biceps femoris
- Long head
- Origin: ischial tuberosity
- Insertion: head of the fibula
- Action: extension of the hip, flexion of the knee
- Innervation: sciatic nerve (tibial portion)
- Short head
- Origin: linea aspera
- Insertion: head of the fibula
- Action: extension of the hip, flexion of the knee
- Innervation: sciatic nerve (fibular portion)
Medial Thigh Muscles
Adductor longus
- Origin: body of pubis
- Insertion: linea aspera
- Action: adduction of the thigh
- Innervation: obturator nerve (L2-4, anterior division)
Adductor brevis
- Origin: body and inferior ramus of pubis
- Insertion: pectineal line
- Action: adduction of the thigh
- Innervation: obturator nerve (L2-4, anterior division)
Adductor Magnus
- Adductor portion
- Origin: inferior pubic ramus
- Insertion: gluteal tuberosity, linea aspera, medial supracondylar line
- Action: adduction and flexion of the thigh
- Innervation: obturator nerve (L2-4, posterior division)
- Hamstring portion
- Origin: ischial tuberosity
- Insertion: adductor tubercle of femur
- Action: adduction and extension of the thigh
- Innervation: sciatic nerve
Gracilis
- Origin: body and inferior pubic ramus
- Insertion: medial surface of tibia via pes anserinus
- Action: adduction of thigh, flexion and medial rotation of the leg
- Innervation: obturator nerve (L2-4, anterior division)
Obturator externus
- Origin: margins of obturator foramen
- Insertion: trochanteric fossa of femur
- Action: lateral rotation of the thigh
- Innervation: obturator nerve (L2-4, posterior division)
Clinical Significance
Understanding the anatomy of the femoral muscles is incredibly important for clinicians to determine a diagnosis for their patients. Muscle pain and weakness can also be signals of a nerve or vessel injury.
Damage to the femoral nerve causes paralysis of the quadriceps, so there are significant deficits in the flexion of the hip and extension of the leg. In cases of obturator nerve damage the patient will present with weakness in adduction and a lateral swinging of the limb during walking there is a lack of opposition to the abductors. When the sciatic nerve is damaged, the extension of the hip and flexion of the knee is impaired, along with several deficits in the foot and ankle. This type of injury can easily be recognized by clinicians because the patient will increase the flexion of the hip to lift the dropped foot off of the ground.
Psoas Abscess
A psoas abscess is a rare clinical diagnosis of an infectious collection of material contained in the psoas muscle. This condition presents with non-specific symptoms including back/flank pain, fever, and weight loss. The most common microorganism is Staphylococcus aureus. The abscess can occur from hematogenous spread with increased risk in patients with diabetes mellitus, IV drug use, AIDS, and renal failure. Additionally, the abscess can form from spreading from a secondary site. This is seen in Crohn's disease or after surgical instrumentation. A positive psoas sign can be seen on examination, in which hip extension increases a patient's pain. The diagnosis is made using ultrasound and CT. The management includes drainage and antibiotic therapy. [9]
Pes Anserine Bursitis
The pes anserine bursa lies between the pes anserine and the medial tibia. The pes anserine is a structure made of the conjoined tendons of the gracilis, semitendinosus, and sartorius. This bursitis is common in middle-aged females. The patient commonly presents with pain on the medial aspect of the knee with tenderness to palpation over the medial tendons at 90 degrees of knee flexion. The management includes rest, ice, and NSAIDs for symptomatic management. [10]
Hamstring Strains
The hamstrings are commonly strained in activities such as running or jumping; these injuries can be very painful. There is a wide range of hamstring injuries that can include strains, complete and partial avulsions, tendinopathy, and referred pain. Of these injuries, hamstring sprains are the most common. Sports with an increased rate of hamstring sprains include football, soccer, rugby, and track as these sports involve the motion of sprinting, kicking, and high-speed movements. Hamstring strains are 64% more likely to occur in a male athlete compared to a female. The injury is managed conservatively and includes rest and physical rehabilitation. [11]
Patella Tendon Reflex
Testing during a physical examination by striking the patellar ligament while the patient is seated with legs dangling. An intact reflex causes the quadriceps muscles to contract and the leg extends. This reflex tests the femoral nerve and the L2-L4 spinal cord segments. [12]
(Click Image to Enlarge)
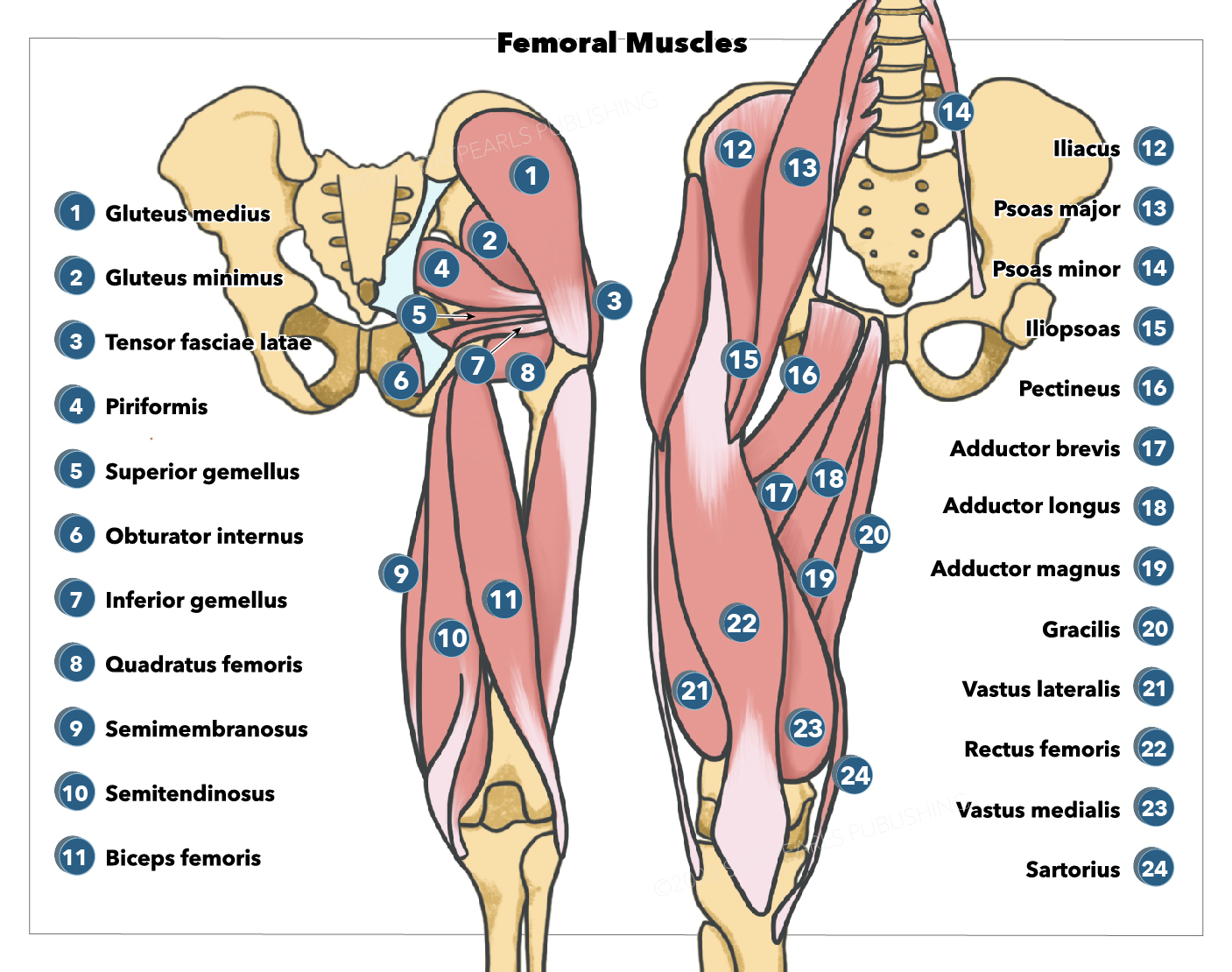
Femoral muscles, Gluteus medius, Gluteus minimus, Piriformis, Superior gemellus, Tensor fasciae latae, Obturator internus, Inferior gemellus, Quadratus femoris, Semitendinosus, Semimembranosus, Biceps femoris, Illiacus, Psoas major, Psoas minor, Iliopsoas, Pectineus, Adductor brevis, Adductor longus, Adductor magnus, Gracilis, Vastus lateralis, Rectus femoris, Vastus medialis, Sartorius
Illustration by Emma Gregory