Neuroanatomy, Pyramidal Tract
- Article Author:
- Qais AbuHasan
- Article Editor:
- Sunil Munakomi
- Updated:
- 7/31/2020 2:56:46 PM
- For CME on this topic:
- Neuroanatomy, Pyramidal Tract CME
- PubMed Link:
- Neuroanatomy, Pyramidal Tract
Introduction
The control of muscular movements in the human brain is very complex yet delicate, multiple areas of the brain are involved, each of which is responsible for specific areas and functions. This control is conveyed mainly through the pyramidal tract, which arises from the pyramidal cell in the cortex, primarily the primary motor cortex. It divides into the corticospinal tract, which synapses with the lower motor neurons innervating the muscles in the limbs and trunk, and the corticobulbar tract, which synapses with the cranial nerves to control muscular movements of the face, head, and neck.
Structure and Function
The pyramidal tract originates from the cerebral cortex, and it divides into two main tracts: the corticospinal tract and the corticobulbar tract, each of those tracts carries efferent signals to either the spinal cord and the brainstem.
The spinal cord receives fibers from the corticospinal tract, which controls the movements in the limbs and trunk. The corticospinal tract originates mainly from the primary motor cortex and premotor area, while also receiving fibers from the somatosensory cortex, cingulate gyrus, and the parietal lobe. Along its descent, it passes through the corona radiata and internal capsule, cerebral peduncles, pons, and upper medulla. Decussation of the fibers (i.e., the crossing of fibers to the opposite side of the body) occurs at the level of the lower medulla, where 85 to 90% of the fibers cross to form the lateral corticospinal tract (LCST). Within the spinal cord, the lateral corticospinal tract descends in the lateral funiculus and terminates at each level of the spinal cord by synapsing with lower motor neurons controlling gross and fine motor movements. Non-decussating fibers continue on the same side within the spinal cord as the anterior corticospinal tract (ACST) and control the proximal muscles as well as the trunk.
The corticobulbar tract is involved in the movement of the face, head, and neck. Its fibers originate in the primary motor cortex and descend similarly to the corticospinal tract through the corona radiata and the internal capsule following which it exits to synapse with the lower motor neurons of the cranial nerves. These fibers innervate all cranial nerve bilaterally except cranial nerves VII and XII, which receive their innervation from the contralateral cortex.[1][2][3]
Embryology
The cerebral cortex gives rise to the corticospinal tract, specifically, the pyramidal cells from layer V in the rostral and frontal parts of the cerebral cortex. Corticospinal projections arise from both the motor and the somatosensory cortices. Despite its importance, the corticospinal tract develops rather late and in a slow process. The tract reaches the level of pyramidal decussation at about eight weeks after fertilization, the development after that is slow, and the myelination of its axons could take up two to three years. Because of this lengthy development, malformations could occur even after birth. The genetic factors involved in tract development are complicated, and much of the process is yet to be known.[4]
Blood Supply and Lymphatics
Each part of the pyramidal tract receives vascular supply by a different artery depending on its anatomical position. The primary motor cortex, from which the pyramidal tract originates, is supplied by the middle cerebral artery (MCA), which is responsible for controlling the face and upper extremities, while the part responsible for the lower extremities gets its supply from the anterior cerebral artery (ACA). Following the course of the pyramidal tract, it passes through the corona radiata and internal capsule, supplied by the lenticulostriate arteries, branches of the MCA themselves. The tract continues to pass down into the brainstem, where the basilar artery provides arterial support. Any blockage to the mentioned arteries will manifest as weakness in the body parts controlled by the areas supplied.[1][5][6]
Physiologic Variants
Autopsy studies done on the pyramidal tract showed many variabilities on many levels of its course, including the pyramidal decussation, which in some cases was absent, while in other cases, there was only partial decussation. Moreover, fibers from each hemisphere could cross at different levels, as those from the left pyramid could decussate at a more cranial level and in higher numbers compared to that on the right side.[4]
Surgical Considerations
Pyramidal tract lesions are identifiable from the set of symptoms presented in the patient and should be managed quickly to avoid devastating consequences. The symptoms could vary depending on the site of the lesion and the tract involved. Spasticity, clonus, and hyperreflexia are a common theme in corticospinal injuries which cause impairment to the movement of the limbs and trunk, which corticobulbar damage cause impaired facial and hypoglossal nerves functions. A detailed history and physical examination will provide enough information to expect the site of injury. With the aid of imaging and other modalities, the insult, if applicable, could be accessed surgically and managed.
The management of these lesions could involve intensive rehabilitation and exercise, medical interventions such a botulinum toxin, and benzodiazepines to decrease spasticity and contractures. Surgery is reserved for severe and life-threatening complications or in those where medical therapy fails to provide relief and improve the quality of life.[7]
Clinical Significance
The pyramidal tract, especially the corticospinal tract, plays a significant role in controlling voluntary muscular movements, and hence, lesions could cause many devastating consequences if severe enough. Different kinds of insults could cause lesions in the pyramidal tract, which include stokes, tumors, hemorrhage, meningitis, trauma, and even multiple sclerosis.
First, understanding the decussation of the corticospinal tract will help to localize anatomical sites based on the clinical signs and symptoms and vice versa. Any damage to the tract above the level of decussation will lead to impairment to the contralateral part of the body, while lesions in the spinal cord below the decussation will manifest in the ipsilateral side. Since the pyramidal tract is a part of the upper motor neuron system, lesions in it will lead to spasticity, hyperreflexia, clonus, and positive Babinski sign.
Meanwhile, lesions in the corticobulbar tract could manifest as pseudobulbar palsy, which presents as slow speech, dysphagia, dysarthria, spastic tongue, or they could manifest as impairment in the function of cranial nerves VII and XII, presenting as contralateral lower facial droop and contralateral weakness in the hypoglossal muscles, respectively.
Diseases that could involve damage to the pyramidal tract include strokes, multiple sclerosis, amyotrophic lateral sclerosis (ALS), central pontine myelinolysis, Friedreich ataxia, and Brown-Sequard syndrome.[2][8][1][9][10]
(Click Image to Enlarge)
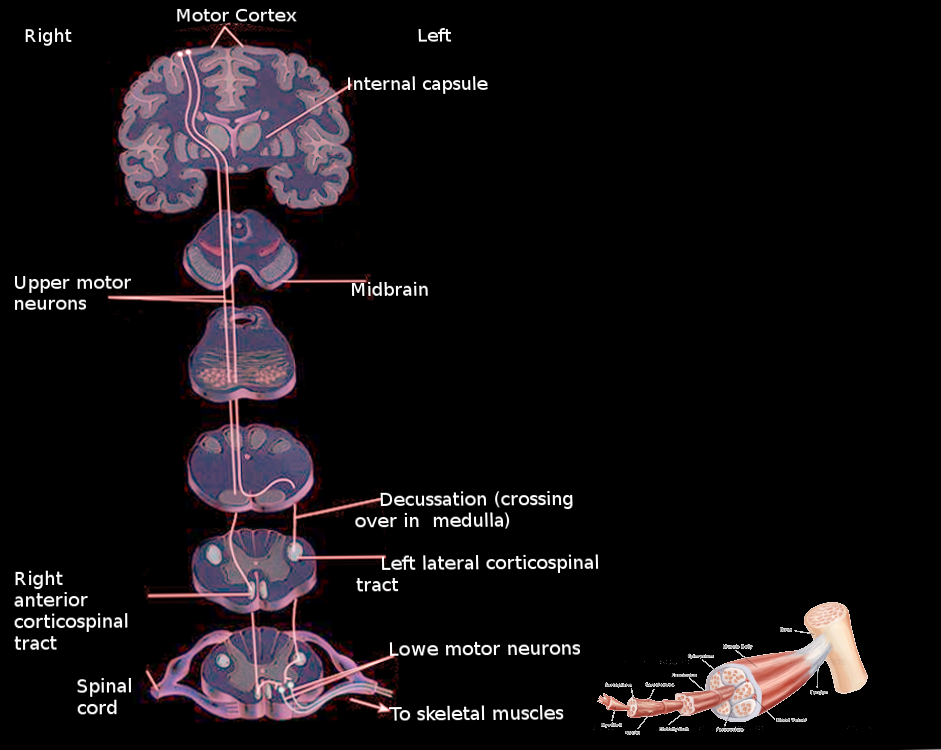
Pyramidal tract
Image courtesy Dr Chaigasame