Anatomy, Angle of Louis
- Article Author:
- Matthew Ball
- Article Author:
- Samuel Falkson
- Article Editor:
- Oluwaseun Adigun
- Updated:
- 7/31/2020 3:59:18 PM
- For CME on this topic:
- Anatomy, Angle of Louis CME
- PubMed Link:
- Anatomy, Angle of Louis
Introduction
The angle of Louis is the eponymous name given to the sternal angle which is the palpable anatomical feature formed from the manubriosternal junction. The manubriosternal junction is the joint of the sternal body and the manubrium.[1][2][3]
This angle of Louis is a synarthrosis, a type of joint characterized as a fibrous connection between two bones (the manubrium and the sternal body in the case of the angle of Louis) which does not allow any significant movement.[4]
In a cadaveric study of preserved skeletal specimens, the sternal angle ranged from 149.0 degrees to 177.0 degrees with an average of 163.4 degrees in men and 165.0 degrees in women.[5]
A small amount of movement in the angle of Louis does occur, particularly in younger people where the fibrous joint features increased flexibility. Complete fusion of the angle of Louis generally occurs at approximately 30 years of age. Using in-vivo spiral-CT data, the movement in the joint during forced breathing has been measured at approximately 4.4 degrees.[6]
Structure and Function
The angle of Louis forms part of the ribcage. It performs generic functions of the skeletal tissues; protection, mechanical leverage for movement, and support for other organs. Importantly, the ribcage provides support for and allows ventilation through movement of the thoracic cage. The movement at the sternal angle allows the body of the sternum to move anteriorly and superiorly. This increases the volume of the intrathoracic cage and in particular, allows transverse expansion in the lower thoracic cage leading to maximal airflow.
Embryology
Blood Supply and Lymphatics
The blood supply to the sternum has been investigated through contrast cross-sectional imaging both in vivo and in cadavers. Cadaveric dissection has added to this knowledge. These studies have revealed the presence of a perforator artery into the sternum at each intercostal level as a branch from the internal mammary arteries. Associated veins have been identified following a similar course.[9] Importantly in patients having internal mammary harvesting, these branches anastomose with the intercostal arteries and therefore indirectly with the posterior intercostal arteries providing a possible collateral blood flow. Despite this structure, studies have still shown that immediately after harvesting of the internal mammary artery there can be a period of ischemia affecting the sternum.[10]
Nerves
The sternum and manubrium are innervated by the intercostal nerves which are part of the somatic nervous system. These nerves arise from the anterior rami of spinal nerves from segments T1-T11. The first two nerves supply the proximal sternum and manubrium. These nerves play a role in the contraction of the intercostal muscles as well as providing sensation to the skin. Unlike the lateral thorax, the manubrium and sternum have fewer nerves- and this explains why a sternotomy incision is less painful than a thoracotomy.
Muscles
The intercostal space superior and inferior to the angle of Louis is spanned by a triple layer of muscle. The outermost intercostal muscles (external intercostals) have fibers running in an oblique direction. These fibers course in an anterior and inferolateral direction and play a role in the elevation of the rib during inspiration. The next set of muscles, the internal intercostals, are also oriented in an oblique fashion, orthogonally to the external intercostals. The innermost set of intercostals are thin and are similar to the internal intercostal muscles in their orientation. In between these runs the neurovascular bundle.
Pectoralis major has its origin across the anterior surface of the sternum and the sternocostal articulations of the superior ribs, and therefore, includes the sternal angle.
Sternalis, a rare anatomical variation, occurs in a single-digit percentage of the population (some estimates pointing to roughly 4%).[11] It commonly originates from the lower costal cartilages as tendinous fibers and runs superiorly parallel to the sternal body, inserting into the sternal angle. A proposed action of sternalis is to help in the expansion of the thoracic cage.
Physiologic Variants
Many different sternal anomalies can occur following abnormal development. A complete sternal cleft can occur when the two sagittal bars of the sternum do not fuse. This can sometimes allow the heart to protrude through the sternum. An incomplete fusion can cause a “sternal foramen” to be left within the sternum.
The sternum can protrude in pectus carinatum (known as pigeon breast due to its similarity to an avian shape of the ribcage). The sternum can also recede in pectus excavatum (known as funnel chest). These variations are due to both abnormal angles of the sternal angle and to curvatures of the sternal body. These abnormalities often become more pronounced during childhood.
Surgical Considerations
Significant pectus excavatum or carinatum is sometimes repaired surgically; these repairs are often performed where the sternal malformation occurs in conjunction with significant scoliosis. However, studies have shown that these repairs do not always lead to improvements in scoliosis and ribcage remodeling.
The manubrium and proximal sternum are routinely opened up during open-heart surgery. Because of the strength of the bone, a mechanical saw is required to access the chest cavity. In children, strong sutures can be used to put the sternum back together, but in all individuals above the age of 2, stainless steel wires are required to realign and close the sternum. If the blood supply to the sternum is poor or if the adjacent ribs have been traumatized, the wires can loosen, and this can result in sternal dehiscence. If there is an infection, the wires may need to be pulled out, and a plastic surgery consult generally must be made so that the sternum can be closed with a muscle flap.
Clinical Significance
The sternal angle is an important clinical landmark for identifying many other anatomical points:
- It marks the point at which the costal cartilages of the second rib articulate with the sternum. This is particularly useful when counting ribs to identify landmarks as rib one is often impalpable. The counting of ribs is essential when one is attempting to make a thoracic incision. If the wrong rib is counted, access to the internal chest organs can be difficult. Additionally, making an incision at the first or second rib interspace can result in damage to large, important blood vessels and the brachial plexus. Identification of the second rib and thus the second intercostal space inferiorly is also useful when auscultating heart sounds. The optimal location for auscultation of the aortic valve is generally the right second intercostal space, whereas the optimal location for auscultation of the pulmonic valve is generally the left second intercostal space.
- It is at the level of the T4-T5 intervertebral disc.
- It marks the level of the transverse thoracic plane which divides the mediastinum into the superior and inferior mediastinum.
- It overlies the aortic arch on the left and the superior vena cava on the right.
- The pericardium extends from just superior to the angle of Louis to the level of the xiphisternal joint.
- It is roughly at the level of the bifurcation of the trachea.
- The tracheal carina is deep to the sternal angle.
- It is roughly at the level of the bifurcation of the pulmonary trunk.
- Ligamentum arteriosum attaches to the aortic arch deep to the angle of Louis.
Other Issues
The source of the eponymous name “the angle of Louis” is believed to have originated from either Antoine Louis, a French clinician, or Wilhelm Friedrich von Ludwig, a German physician. However, there is no definitive evidence of either origin, and some speculation even suggests it originates from another doctor, Pierre Charles Alexandre Louis.
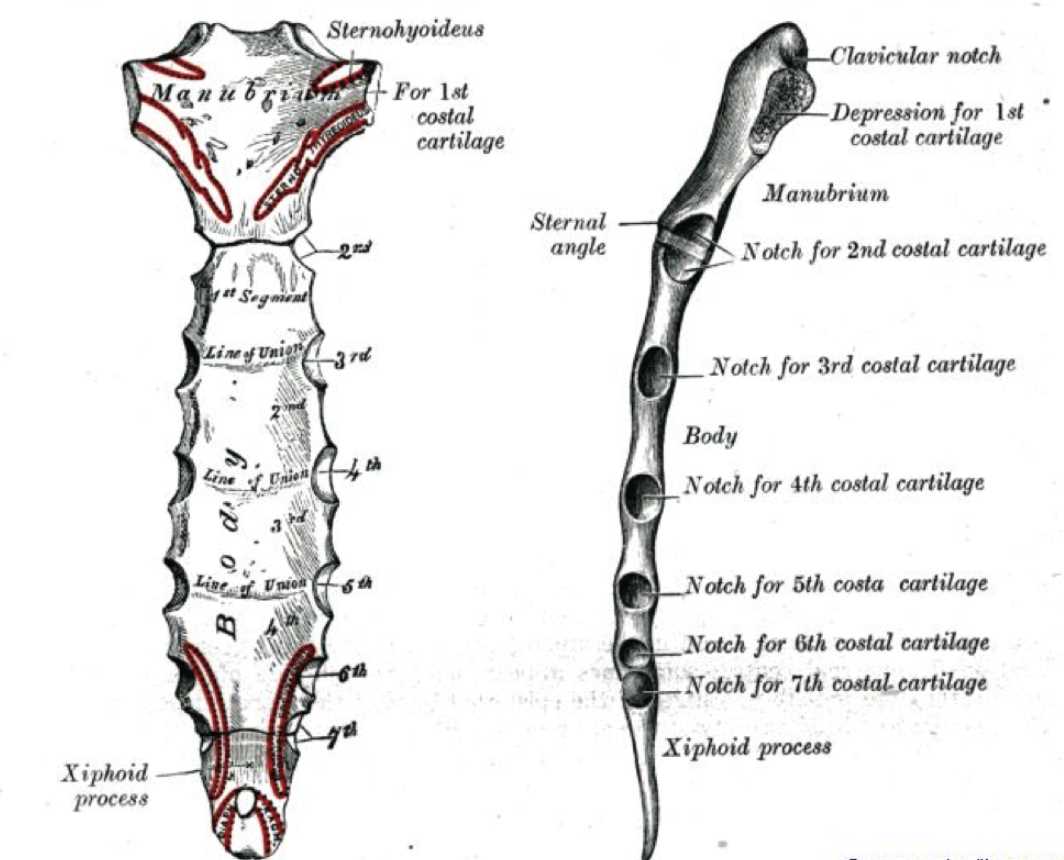
(Click Image to Enlarge)

Sternum, Jugular Notch, Manubrium, Sternal Angle, Body, Xiphoid Process, Clavicular Notch, Facets for Attachment of Costal Cartilages 1-7
Contributed Illustration by Beckie Palmer
(Click Image to Enlarge)
Sternum, Angle of Louis, Manubrium
Contributed by William Gossman Collection