Ear Nerve Block
- Article Author:
- Linda Kravchik
- Article Author:
- Matthew Ng
- Article Editor:
- Tess VanHoy
- Updated:
- 10/3/2020 10:14:49 AM
- For CME on this topic:
- Ear Nerve Block CME
- PubMed Link:
- Ear Nerve Block
Introduction
Patients frequently present to the emergency department with a variety of external ear complaints ranging from traumatic injuries (lacerations and avulsions), auricular collections that require drainage (hematomas and abscesses) and embedded foreign bodies (earrings and earring backings). Typically, oral and parenteral medications do not provide adequate pain relief, and procedural sedation has a sizeable risk burden particularly in pediatric patients. Injections directly into the external ear are painful and have a high risk of provider needlestick. On the other hand, if a larger area of analgesia for the ear is needed, a peripheral nerve block is typically a well-tolerated method. Multiple nerves innervate the external ear and originate from both cranial nerves and the cervical plexus. Historically, the ring block was the most common method of peripheral external ear nerve block. With the increased availability and use of ultrasound in the emergency department, the literature shows that ultrasound can help localize the great auricular nerve and the lesser occipital nerve for nerve block. Additional nerve block of the auriculotemporal nerve is as, if not more effective, more direct, and provides equivalent analgesia using less anesthetic agent.
Anatomy and Physiology
External ear anatomy ear includes the external auditory canal, auricle or pinna (comprised of the helix, antihelix, and lobule), the antitragus, the tragus, and the concha. The sensory innervation arises from the great auricular and lesser occipital nerves both branches of the second (C2) and third (C3) branches of the cervical plexus, the auriculotemporal nerve from the mandibular branch of the trigeminal nerve and the auricular branch of the vagus nerve known as Alderman's or Arnold's nerve. More specifically, the great auricular nerve is derived from the cervical plexus (C2, C3), coursing around the posterior aspect of the sternocleidomastoid muscle and becomes most superficial at the level approximately 6 to 7 cm below the external auditory meatus. It arborizes into an anterior and posterior branch toward the front and underside of the ear, respectively. The lesser occipital nerve (C2, C3) courses around the posterior edge of the sternocleidomastoid at the level approximately 4 to 5 cm below the external auditory meatus and heads toward the backside of the ear. The auriculotemporal nerve takes its origin from the 3rd branch of the trigeminal nerve, the mandibular nerve. The nerve ascends in front of the ear anterior to the tragus. The auricular branch of the vagus nerve exits the temporal bone at the tympanomastoid suture, deep in the concha.
Sensory innervation to the auricle is regional. The helix, concha, and lobule receives its innervation from the great auricular nerve. The antihelix, antitragus, tragus, and concha are innervated by mainly the great auricular nerve and to a lesser degree the auricular branch of the vagus nerve. The superomedial helix (the crus and spine) is innervated primarily by the auriculotemporal nerve. The backside of the auricle is innervated by three nerves: the great auricular nerve, lesser occipital nerve and auricular branch of the vagus nerve. Variable sensory distributions and patterns between these nerves have been described. [1]
Indications
In the emergency department, a nerve block of the external ear is most suitable for, but not limited to the following situations[2][3][4]:
- Analgesia to allow for a more thorough exam and repair of the external ear in trauma
- Patients with contraindications to general anesthesia and procedural sedation
- Incision and drainage, followed by packing of an auricular hematoma
- Incision and drainage of abscesses and cysts
- Laceration repair
- Foreign body removal
- Red ear syndrome
- Great auricular neuralgia
Contraindications
- Known anesthetic agent allergy
- Uncooperative patient
- Cellulitis or erythema overlying the injection site (relative contraindication due to the theoretical risk of spreading the infection)
- Coagulopathy
Equipment
Ring Block requires the following[1]:
- Sterile gloves
- Surgical mask with eye protection/goggles
- Anesthetic agent: 0.5% bupivacaine or 1% lidocaine with or without epinephrine*
- 25 or 27 gauge 1.5-inch needle
- 10 mL syringe
- Chlorhexidine 2%
- Sterile 4 x 4 gauze
Ultrasound-guided greater auricular nerve block requires the following[5][6]:
- Sterile gloves
- Surgical mask with eye protection/goggles
- Anesthetic agent: 0.5% bupivacaine or 1% lidocaine with or without epinephrine*
- 25 or 27 gauge 1.5-inch needle
- 10 mL syringe
- Chlorhexidine 2%
- Sterile 4 x 4 gauze
- Ultrasound machine with a high-frequency linear probe
- Sterile ultrasound gel
*historically, the addition of epinephrine to local anesthetic injected into the auricle was contraindicated but recent literature demonstrates its safety without risk of ischemic necrosis[7][8]
Personnel
Medical professionals to include physicians, physician assistants and nurse practitioners who are trained and experienced in the performance of peripheral nerve blocks, as well as, skilled in ultrasound-guided procedures. One nonsterile person for assistance as needed.
Preparation
Explain the risks and benefits of a peripheral nerve block to the patient and obtain written informed consent if the patient is able. Lay the patient in lateral decubitus position with the affected side up. Set the ultrasound machine on the opposite side of the stretcher from where you will be standing. Sterilize the linear ultrasound probe and place in a sterile probe cover. Cleanse the area of the auricle (both anterior and posterior surfaces), the postauricular area including the mastoid process, front of the ear, and the lateral neck along the sternocleidomastoid muscle with 2% chlorhexidine. Drape the patient with sterile towels with prepped area exposed. Let the chlorhexidine dry completely before beginning the procedure. Apply sterile ultrasound gel to the area.
Technique
Ring Block:
- Insert the 25G, 1.5 inch needle subcutaneously below the earlobe in line with the external auditory meatus
- Aspirate before injecting to ensure that vascular injection (specifically the posterior auricular and superficial temporal arteries) does not occur
- Inject 1mL of anesthetic agent into the spot of needle entry
- Direct the needle behind the ear towards and over the mastoid process 2 - 4 mm deep and advance it parallel to the skin to about full length of the needle and inject approximately 2mL of anesthetic as you withdraw the needle
- Stop short of taking the needle out of the skin when back to the first position
- Direct the needle anterior to external ear towards the area just in front of the tragus, aspirate, then inject another 2mL as you withdraw the needle completely
- Insert the needle subcutaneously directly above the ear again in line with the external auditory canal
- Repeat steps 2 through 6 but with the needle facing caudally towards and over the mastoid process and immediately anterior to the tragus
At completion, typically, the total amount of local anesthetic is approximately 10 to 12mL, and the trajectory of the injections will look like a V (for the inferior ear block) and an upside-down V (for athe superior ear block) encircling the ear.
Ultrasound-guided Great Auricular and Lesser Occipital Nerve Block:
- With the linear ultrasound probe in the transverse orientation, place it at the middle of the sternocleidomastoid and track slowly upward towards the earlobe along the posterior edge of the sternocleidomastoid until you see two hypoechoic nerve structures approximately 4 to 5 cm inferior to the ear
- Insert the needle in-plane so that you can visualize the tip of the needle on the screen
- Advance needle slowly until it is almost at the nerve - do not inject into the nerve
- Aspirate and then inject 1 to 2mL into the space between the needle tip and the nerve
NOTE: To quickly access the great auricular nerve as it courses across the sternoicleidomastoid muscle using external topographic landmarks, the great auricular nerve is located at junction of the upper one-third and lower two-third of the muscle between the mastoid process and clavicle.[9]
NOTE: To obtain complete anesthesia of the external ear particularly the superior-medial helix minus the external canal you will have to perform steps 7 and 8 of the ring block (to include the auriculotemporal nerve distribution) with the great and lesser occipital nerve block.
NOTE: The ring block provides analgesia for the external ear with the exception of the external auditory canal.
Complications
- Pain
- Bleeding
- Infection
- Allergic reaction to the anesthetic agent
- Hematoma formation
- Injury to surrounding vasculature
- Systemic anesthetic toxicity
- Inadvertent injection of facial nerve leading to temporary facial paralysis
Clinical Significance
Peripheral nerve block of the external ear is a valuable procedure utilized in a multitude of settings including the operating room, office, and emergency department. It is a well-tolerated, relatively quick procedure that can be used on its own or as an adjunct to other forms of analgesia.
Enhancing Healthcare Team Outcomes
Expeditious, humane and safe care of patients should always guide us in our practice. Peripheral nerve block of the external ear is a valuable procedure to become familiar with as it can expedite analgesia which will then accelerate completion of procedures and decrease patient discomfort whether suturing a laceration, draining an abscess, or removing a foreign body. By utilizing the peripheral nerve block, patient-centered care is at the forefront as it minimizes pain quickly and more safely than injecting directly into the external ear. The peripheral nerve improves safety with fewer needle-sticks to health professionals compared to direct local injection and shorter overall procedure duration utilizing fewer staff members when compared to moderate sedation or general anesthesia. The use of ultrasound improves locating the nerves, avoids vasculature and decreases the amount of anesthetic required.
(Click Image to Enlarge)
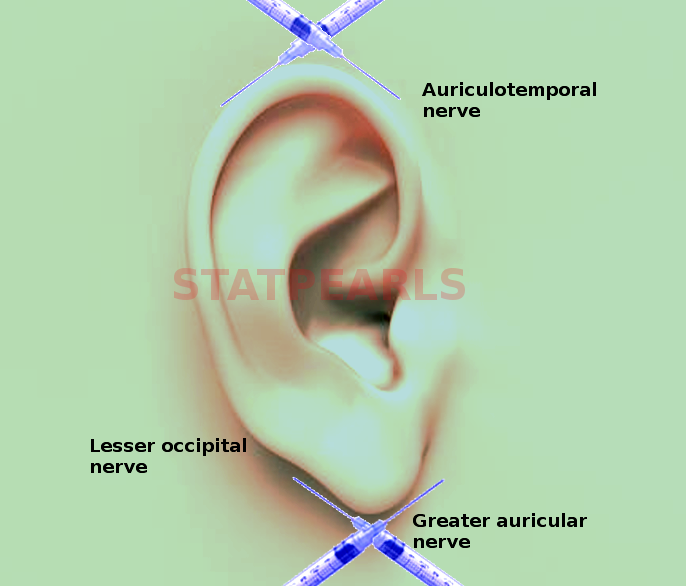
Ear nerve block
Image courtesy S Bhimji MD