Anatomy, Head and Neck, Eye Superior Tarsal Muscle (Mullers Muscle)
- Article Author:
- Ahmed Abdelhady
- Article Editor:
- Bhupendra Patel
- Updated:
- 9/16/2020 10:04:15 AM
- For CME on this topic:
- Anatomy, Head and Neck, Eye Superior Tarsal Muscle (Mullers Muscle) CME
- PubMed Link:
- Anatomy, Head and Neck, Eye Superior Tarsal Muscle (Mullers Muscle)
Introduction
The superior tarsal muscle, known as Muller’s muscle, is a structural muscle which functions to maintain the elevation of the upper eyelid. It receives innervation from the sympathetic nervous system and is unique in that it consists of thin fibers of the smooth muscle. Damage to this muscle, or the nerves which supply it, will result in ptosis of the affected eye as seen in Horner syndrome, a condition in which there is damage to the cervical sympathetic chain. Surgeries which involve repair of ptosis, or upper eyelid correction procedures, will usually encounter Muller's muscle and should be very precise in adjustments when resecting portions of the upper eyelid.
Structure and Function
The structure of the superior tarsal muscle is unique in that it adjoins and originates from underneath another muscle, the levator palpebrae superioris. The superior tarsal muscle is visible with the naked eye and is about 15 mm wide by 10 mm long. It is made of thin fibers of smooth muscle tissue and, after originating from underneath the levator palpebrae superioris muscle, it reaches its insertion point on the superior tarsal plate of the upper eyelid. This plate is made of dense connective tissue and functions to maintain form and support the upper eyelid.[1]
The superior tarsal muscle has a unique function in that it assists the levator palpebrae superioris by maintaining the elevation of the upper eyelid after the levator palpebrae superioris has raised it.[6] The superior tarsal muscle also functions to raise the upper eyelids an additional 2 mm after the levator palpebrae superioris has already initially raised them as a sympathetic nervous system response.[1]
The superior tarsal muscle was found to have a much more significant role in levator action when compared to the levator palpebrae superioris than previously thought. Research has determined that the superior tarsal muscle transmits a considerable amount of power to the levator palpebrae superioris when elevating the eyelid.[2]
Embryology
The superior tarsal muscle develops in a way, not unlike the other extraocular muscles. These subtype of muscles are different in that; when compared to periocular tissues, these muscles came from paraxial mesoderm in the prechordal plate, which is unusual in that connective tissue tendons arise from neural crest cells instead. Specifically, around week five is when Muller's muscle first appears in development.[3]
Blood Supply and Lymphatics
Oxygenated blood reaches the superior tarsal muscle through the lateral muscular branch of the ophthalmic artery. This branch also supplies blood to the lateral rectus, superior rectus, superior oblique, and levator palpebrae muscles. The ophthalmic artery also has a medial muscular branch supplying blood to the remaining extraocular muscles.
The superior tarsal muscle drains deoxygenated blood into the same veins as the remaining extraocular muscles. These veins, known as vortex veins - originating from the posterior part of the eye, are where the blood leaving the superior tarsal muscle reaches first. This blood then drains into the superior and inferior orbital veins which eventually reach the cavernous sinus.
Nerves
The innervation of the superior tarsal muscle is from the sympathetic nervous system. Specifically, postganglionic sympathetic fibers originating from the superior sympathetic cervical ganglion reach the muscle by forming fibers. These fibers wrap around the carotid artery as the pericarotid plexus and enter the skull, reach the cavernous sinus, and then access the orbit to reach the muscle.[4]
Muscles
The specific muscle subtype of the superior tarsal muscle is different from the other extraocular muscles. The superior tarsal muscle is made up of smooth muscles, specifically thin fibers of smooth muscular tissue. This muscle originates at the underside of the levator palpebrae superioris and attaches to the superior tarsal plate.[2]
Specific differences which are seen in this muscle compared to other smooth muscles exist. One such difference is the fact that the superior tarsal muscle is made up not solely of smooth muscle but instead is mixed tissues. These tissues include connective tissue, blood vessels, and fat. Also, one key difference between the superior tarsal muscle and others is that the smooth muscle cells of this muscle are distributed sporadically and are not attached to each other. Lastly, another difference shows that the origin of the superior tarsal muscle may contain fibers of striated muscle connected with fibers of the smooth muscle.[2]
Physiologic Variants
The superior tarsal muscle has specific physiologic variants when comparing different individuals, and these center around the attachment of the muscle to the superior tarsal plate. Four variations exist, and they are below:
- The superior tarsal muscle attaching to the upper border of the superior tarsal plate
- 2M: The superior tarsal muscle attaches to the medial aspect of the plate
- 2L: The superior tarsal muscle attaching to the lateral aspect of the plate
- The superior tarsal muscle attaches along the whole extent of the superior tarsal plate.
The third variation was the most frequently observed variation.[5]
Surgical Considerations
Specific surgeries that encounter the superior tarsal muscle include procedures focusing on correction of elevation dysfunctions of the upper eyelid. These surgeries usually resect the superior tarsal muscle and the levator palpebrae superioris muscle together. A 10-year study of this procedure found that, after resecting the superior tarsal muscle, a significant majority of patients with congenital and acquired ptosis were within 1.5 mm of the opposite lid level, and less than 1% required additional surgery.[6]
Another specific surgery which affecting the superior tarsal muscle is the superior tarsal muscle-conjunctival resection procedure. When performing this procedure, intended for correction of ptosis, careful consideration is to be given to adjustments of the resection, which is usually by resecting a very small amount per elevation required from the superior tarsal border. It is in this situation where the physiologic variants mentioned above are helpful to understand.[7]
Clinical Significance
Since the function of the superior tarsal muscle is to maintain the elevation of the eyelid, it is then easy to understand that damage to this muscle will result in ptosis of the affected eye. In addition, after recognizing that the innervation of the muscle is through the sympathetic nervous system, it is then clear to see that damage to the sympathetic nervous system will also cause ptosis.
One clinical situation in which the sympathetic nervous system innervating the superior tarsal muscle is affected is Horner syndrome. This is a condition in which a structural lesion in the cervical sympathetic chain causes specific symptoms such as upper eyelid ptosis, miosis, and anhidrosis on the ipsilateral side of the lesion. There is paralysis of the superior tarsal muscle in this pathology.[2]
One condition in which the superior tarsal muscle is hyperactive is exophthalmia, a condition associated with hyperthyroidism.[1]
(Click Image to Enlarge)
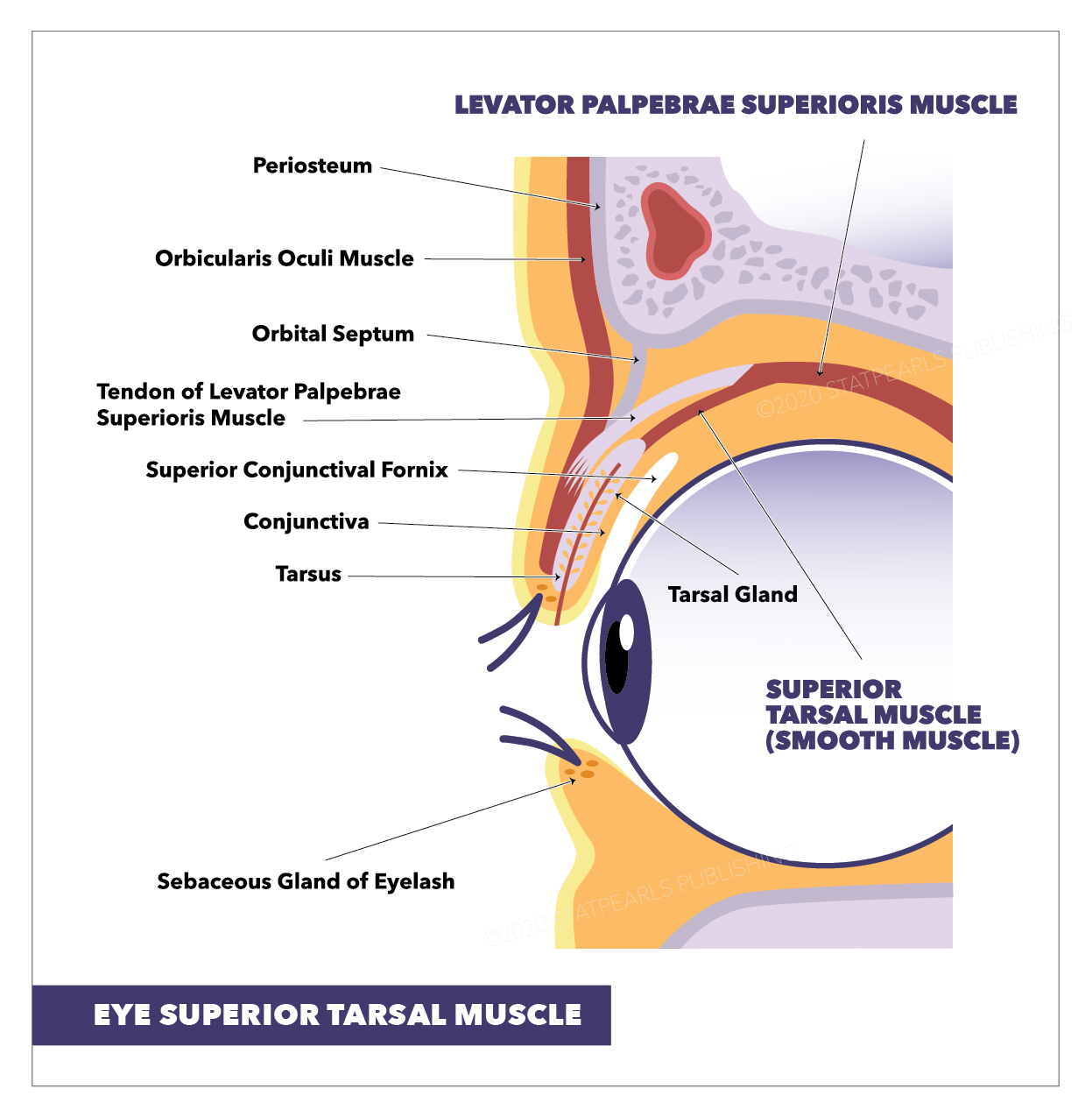
Eye Superior Tarsal Muscle: Tarsal Gland, Levator Palpebrae Superioris Muscle, Sebaceous Gland of Eyelash, Tarsus, Conjunctiva, Superior Conjunctival Fornix, Tendon of Levator Palpebrae Superioris Muscle, Orbital Septum, Superior Tarsal Muscle (SMOOTH MUSCLE), Orbicularis Oculi Muscle, Periosteum
StatPearls Publishing Illustration