Anembryonic Pregnancy
- Article Author:
- Khalid Chaudhry
- Article Author:
- Dawood Tafti
- Article Editor:
- Marco Siccardi
- Updated:
- 8/10/2020 5:43:41 PM
- For CME on this topic:
- Anembryonic Pregnancy CME
- PubMed Link:
- Anembryonic Pregnancy
Introduction
An anembryonic pregnancy is characterized by a gestational sac that forms and grows while an embryo fails to develop. Although the terms anembryonic pregnancy and blighted ovum are synonymous, the latter is falling out of favor for the more descriptive former term. Anembryonic pregnancy constitutes a significant but unknown proportion of miscarriages with the American Pregnancy Association estimating anembryonic pregnancy to constitute half of all first trimester miscarriages. Approximately 15% of all clinically recognized pregnancies end in first-trimester loss with live birth occurring in only 30% of all pregnancies. [1][2] A significant proportion of patients with early pregnancy loss(that include anembryonic pregnancies) are unaware of their miscarriage particularly when early pregnancy loss occurs in the early stages of pregnancy.
In the first trimester, the terms early pregnancy loss, miscarriage, or spontaneous abortion are often used interchangeably. Early pregnancy loss is defined as the spontaneous loss of a pregnancy before 13 weeks of gestation.[3][4]
What is a Miscarriage?
The World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) define miscarriage as the loss of a pregnancy before 20 weeks of gestation or the ejection or removal of an embryo or fetus that weighs 500 g or less. This definition is used in the United States; however, it may vary based on State laws.[5]
Biochemical miscarriage is a loss that occurs after a positive urine pregnancy test (hCG) or a raised serum beta-hCG before ultrasound or histological verification and confirmation.
Clinical miscarriage is when ultrasound examination or histologic evidence has confirmed the existence of an intrauterine pregnancy. Clinical miscarriage is classified as early (before 12 weeks of pregnancy) and late (12 weeks to 20 weeks).
Etiology
The exact etiology for anembryonic pregnancies is difficult to ascertain. The etiological factors for anembryonic pregnancies are generally understood and studied in the broader context of early pregnancy loss (EPL) which includes both embryonic and anembryonic pregnancies. Etiologies include:
- Morphological abnormalities of an embryo that prevents implantation or prevents long term survival of the embryo after implantation. These morphological abnormalities are thought to be related to chromosomal abnormalities. [6]
- Chromosomal abnormalities that collectively include autosomal trisomy, polyploidy, sex chromosomal polysomy, and monosomy X likely represent the most common etiologies for EPL. Trisomies are the major fetal chromosomal abnormality in sporadic cases of miscarriage (30% of all miscarriages) and 60% of chromosomally abnormal miscarriages (recurrent miscarriage). Trisomies with monosomy X (15% to 25%) and triploidy (12% to 20%) account for over 90% of all chromosomal abnormalities found in sporadic cases of miscarriage. According to a study by Edmonds in 1992, trisomy 16 was found to give rise to rudimentary embryonic growth with an empty sac, while other trisomies often resulted in early embryonic demise.
- Other genetic and chromosomal abnormalities include translocations, inversions, single-gene perturbations, and placental mosaicism. [7] Consanguineous marriages resulting in anembryonic pregnancies have also been noted, suggesting a role of single gene determinants. [8] There is a probable link between DNA damage in sperm and miscarriage. [9]]
- Obesity and advanced maternal age are well-established factors associated with early pregnancy loss. [10]
- Tuberculosis in the developing world as well as reproductive tract infections worldwide can predispose to EPL. [11] The complications of genital tract infections that include intrauterine adhesions can impede implantation and embryo growth.
- Malformation of the uterus that includes didelphic, bicornuate, and septate uteri can impede in or prevent the longterm implantation of an embryo.
- Immunologic disorders in the mother such as NK Cell Dysfunction, autoantibodies, hereditary, and acquired thrombophilia, among others) can lead to the maternal immunological rejection of the implanting embryo in the uterus resulting in miscarriage.
- Hormonal factors (such as low levels of progesterone) and endocrinological disorders(thyroid autoimmunity and thyroid dysfunction) play a complex role in miscarriage. Polycystic ovarian syndrome is also associated with infertility and pregnancy loss.
- The role of alcohol consumption and it's associated increased risk in miscarriage has been well established. [12]
Epidemiology
Although difficult to definitively establish, anembryonic pregnancy possibly represents half of all miscarriages in the first trimester of pregnancy. [13][14] The incidence of early pregnancy loss (before 12 weeks) is estimated to be about 15% of clinically evident conceptions with significant variations in incidence based on patient age. The incidence ranges from 10% in women 20 to 24 years of age to 51% in women 40 to 44 years of age. [15] A prior history of early pregnancy loss also predisposes a patient to miscarriage. [16]
History and Physical
The signs and symptoms of an anembryonic pregnancy can potentially mirror those of an ectopic pregnancy. Anembryonic pregnancy is often incidentally noted on an initial first-trimester pregnancy sonogram. If an anembryonic pregnancy progresses to an early pregnancy loss, the patient can present with abdominal cramping and vaginal bleeding. Early pregnancy loss in the setting of an anembryonic pregnancy can be clinically silent.
Evaluation
Clinical signs and symptoms, a pregnancy test, and an ultrasound exam confirm the diagnosis.
A pregnancy test can be obtained using urine or serum hCG levels.
Ultrasound exam (transabdominal or transvaginal) classically demonstrates an empty gestational sac without an embryo.
An anembryonic pregnancy is established on endovaginal ultrasound technique when there is no discernable embryo seen in a gestational sac with a mean sac diameter of ≥25 mm.
Alternatively, an anembryonic pregnancy can be established when there is no embryo on a follow-up endovaginal scan:
- ≥11 days after a scan demonstrating a gestational sac with a yolk sac, but an absent embryo
- ≥ 2 weeks (14 days) after a scan demonstrating a gestational sac without an embryo or a yolk sac
Treatment / Management
The three treatment options for early pregnancy loss include expectant management, medical management, and surgical treatment. Medical management with misoprostol and surgical treatment is considered more effective in the management of anembryonic pregnancy. Ultimately the decision on considering one of these options is based on an informed conversation between a patient and the provider.
- Expectant management
- This constitutes the "watchful waiting" approach
- The patient is closely followed without intervention for spontaneous and complete passage of tissue
- Repeat sonograms and trending hCG levels are employed to confirm complete passage of tissue
- A reasonable determination of a downtrending hCG is sufficient
- Medical management
- This employs misoprostol(an analog of prostaglandin), 800 mcg, administered vaginally
- Optimal dosage is an ongoing area of research
- This management option allows for a more predictable treatment course
- Surgical Treatment
- Surgical management employs uterine evacuation with a manual vacuum
- Frequently employed in patients with hemodynamic instability
- Uterine aspiration/evacuation is quicker to complete, especially when performed on an outpatient basis
Differential Diagnosis
The chief obstetric differential diagnosis for an anembryonic pregnancy includes:
- Pseudogestational sac which represents a small amount of intrauterine fluid
- Early intrauterine pregnancy
- An ectopic pregnancy
- Implantation bleeding from an otherwise viable pregnancy
- Gestational trophoblastic disease
- Complications relating to a viable pregnancy
Prognosis
Prognosis and successful management of early pregnancy loss depends on a variety of factors including gestation age. Prognosis is generally considered good with all three management options.
- Expectant management: in a meta-analysis of 20 studies, expectant management and medical management were both determined to be acceptable treatment options for incomplete abortion. [17]
- Medical management: medical management is more successful with multiple-dose regimens of misoprostol. Patients with incomplete abortion are treated more successfully with medical management than with expectant management.
- Surgical Treatment: at least one large randomized control trial determined a higher success rate in surgical treatment than with medical management, with a general conclusion of the general safety of both treatment options. [18]
Complications
Serious complications of treatment are uncommon. Complications can include:
- Heavy bleeding/hemorrhage
- Uterine perforation(from surgical management)
- Infection to include fatal sepsis
- Complications from a missed ectopic pregnancy
Consultations
- OB/GYN
- Primary care provider
- Psychologist/psychiatrist
- Emergency department physician
- Radiologist/sonographer(especially when there is a concern for an ectopic pregnancy)
Deterrence and Patient Education
The following represent key points in patient education:
- Patients should be advised to present to their emergency department if they experience heavy vaginal bleeding(two pads per hour for approximately two consecutive hours).
- Signs and symptoms of infection should be discussed with patients especially following surgical management.
- Treatment with misoprostol can cause a febrile reaction which can be misinterpreted as a sign of infection.
- Prophylactic antibiotics are not routinely administered but can be considered in select patients.
- Patients should adhere to follow-up sonogram and outpatient appointments especially when additional doses of misoprostol are considered to be clinically necessary.
- A miscarriage can be a traumatic experience for a patient. Reassurance and empathy play a key role in helping patients through the grieving process.
Pearls and Other Issues
- Pregnancy loss is a common complication in the first trimester of pregnancy
- Most losses occur in the first trimester
- Early pregnancy loss without embryo development is likely due to chromosomal and genetic abnormalities
- There are specific sonographic criteria for determining an anembryonic pregnancy
- A pseudogestational sac, an ectopic pregnancy, and an early pregnancy are important differential diagnoses to consider when evaluating an anembryonic pregnancy
- Expectant management, medical treatment with misoprostol, and surgical treatment are the three primary options for management
Enhancing Healthcare Team Outcomes
Establishing an anembryonic pregnancy can sometimes b difficult on an ultrasound. Communication with the radiologist relaying hCG lab values and patient presentation can be helpful in avoiding a missed diagnosis of an ectopic pregnancy. The sonographer also plays an important role in accurately evaluating a patient to appropriately exclude an ectopic pregnancy. Patients presenting with complications of either initial presentation or from treatment often present to the emergency department. Interprofessional communication between an emergency department provider and an OB/GYN specialist includes communicating a detailed and thorough history and physical exam. This especially includes signs of sepsis or hemodynamic instability. The role of a mental health professional in following up with patients is also critical in ensuring the appropriate mental health management of a possibly traumatic experience for a patient.
(Click Image to Enlarge)

Blighted Ovum, ultrasound
Contributed by Tripthi M. Mathew, MD, MPH, MBA, PhD.
(Click Image to Enlarge)
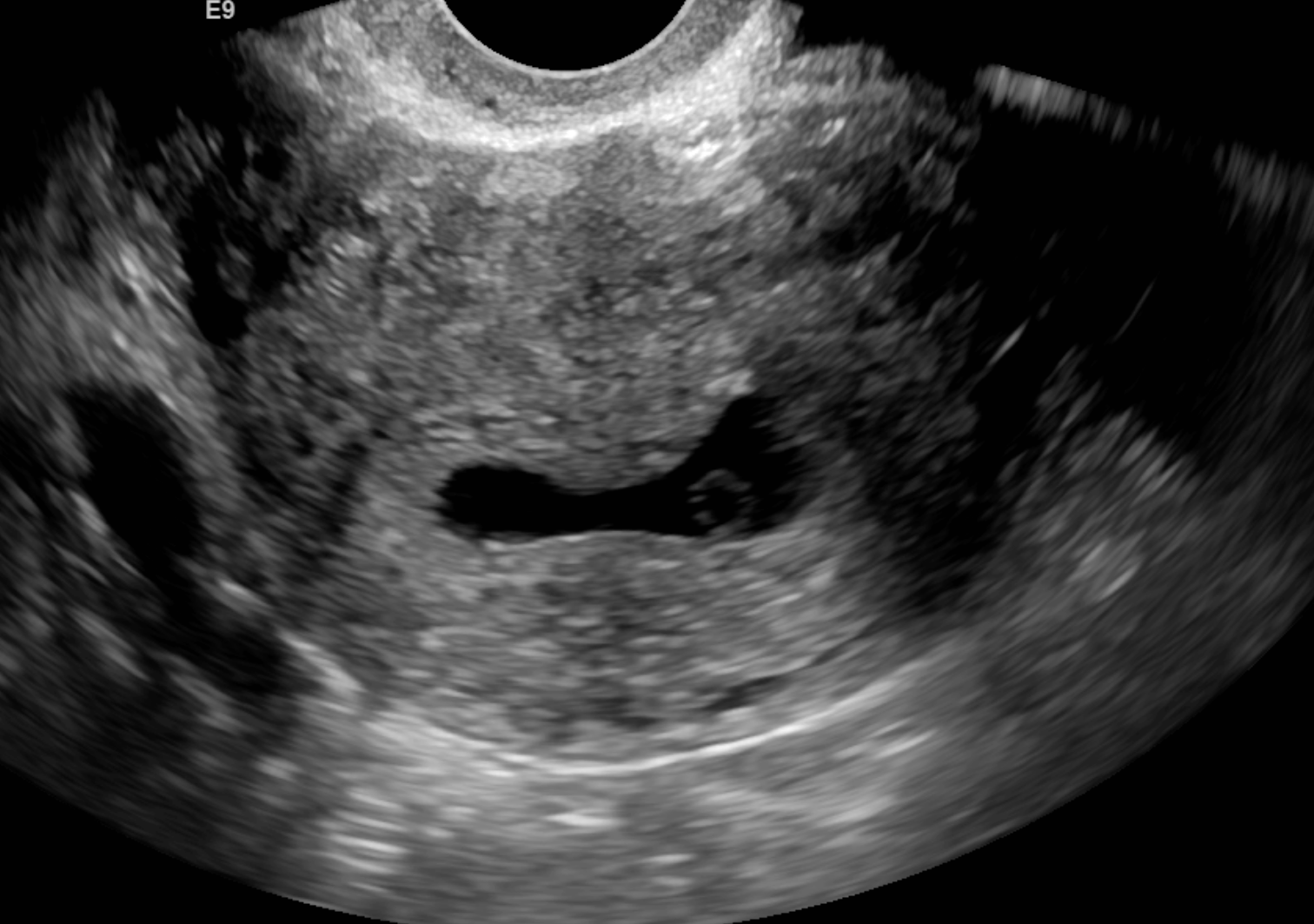
Single sonographic image demonstrating a gestational sac with a yolk sac. No fetal pole is seen. This is representative of a blighted ovum.
Contributed by Dr.Dawood Tafti, MD.
(Click Image to Enlarge)

Single sonographic image demonstrating a gestational sac with a yolk sac. No fetal pole is seen. This is representative of a blighted ovum.
Contributed by Dr.Dawood Tafti, MD
(Click Image to Enlarge)

Single sonographic image demonstrating a gestational sac with a yolk sac. No fetal pole is seen. This is representative of a blighted ovum.
Contributed by Dr.Dawood Tafti, MD.