Drug Enforcement Administration Drug Scheduling
- Article Author:
- Michael Lopez
- Article Editor:
- Prasanna Tadi
- Updated:
- 9/25/2020 12:21:22 PM
- For CME on this topic:
- Drug Enforcement Administration Drug Scheduling CME
- PubMed Link:
- Drug Enforcement Administration Drug Scheduling
Definition/Introduction
Drug scheduling became mandated under The Federal Comprehensive Drug Abuse Prevention and Control Act of 1970 (also known as the Controlled Substances Act). The law addresses controlled substances within Title II. Based upon this law, the United States Drug Enforcement Agency (DEA) maintains a list of controlled medications and illicit substances that are categorized from scheduled I to V. The five categories have their basis on the medication’s proper and beneficial medical use and the medication’s potential for dependency and abuse. The purpose of the law is to provide government oversight over the manufacturing and distribution of these types of substances. Prescribers and dispensers are required to have a DEA license to supply these drugs. The licensing provides links to users, prescribers, and distributors.[1][2][3]
Issues of Concern
The schedules range from Schedule I to V. Schedule I drugs are considered to have the highest risk of abuse while Schedule V drugs have the lowest potential for abuse. Other factors considered by the DEA include pharmacological effect, evidenced-based knowledge of the drug, risk to public health, trends in the use of the drug, and whether or not the drug has the potential to be made more dangerous with minor chemical modifications.
Schedule I:
- "High abuse potential with no accepted medical use; medications within this schedule may not be prescribed, dispensed, or administered"[1]
- Examples of include marijuana (cannabis), heroin, mescaline (peyote), lysergic acid diethylamide (LSD), methylenedioxymethamphetamine (MDMA), and methaqualone.
Schedule II:
- "High abuse potential with severe psychological or physical dependence; however, these medications have an accepted medical use and may be prescribed, dispensed, or administered"[1]
- Examples include fentanyl, oxycodone (OxyContin), morphine, methylphenidate (Ritalin), hydromorphone (Dilaudid), amphetamine (Adderall), methamphetamine (meth), pentobarbital, and secobarbital.
- schedule II drugs may not receive a refill
Schedule III:
- "Intermediate abuse potential (i.e., less than Schedule II but more than Schedule IV medications)"[1]
- examples include anabolic steroids, testosterone, and ketamine
Schedule IV:
- "Abuse potential less than Schedule II but more than Schedule V medications"[1]
- examples include diazepam (Valium), alprazolam (Xanax), and tramadol
Schedule V:
- "Medications with the least potential for abuse among the controlled substances." [1]
- examples include pregabalin (Lyrica), Diphenoxylate/atropine (Lomotil), dextromethorphan (Robitussin)
See Table 1 for information regarding registration, records, prescriptions, refills, distribution, security, and theft or significant loss of controlled substances.
See Table 2 for information regarding DEA forms 106, 222, 224, and 224a.
Clinical Significance
Medications are routinely added to the list and can be moved from one category to another as our knowledge and understanding of the medications advances. The DEA maintains a current list on its website under the diversion control division heading. Prescribers may prescribe, as allowed by their DEA and state controlled-substance or medical license, Schedule II through V medications. Not all prescribers are licensed to prescribe all levels of controlled substances as their individual state or DEA licenses limit some, and some are under limitations by their professions, such as advanced practice providers in many states. It is the responsibility of the provider and the dispensing pharmacist to be aware of each medication's category and ensure that only properly licensed individuals are prescribing the medications. It is essential to understand the DEA controlled-substance scheduling both to ensure adequate caution when prescribing medications with high abuse potential and also to ensure against prescribing outside of one's authority.[4][5]
The Controlled Substances Act has great potential to improve patient safety by providing federal oversight for drugs with a high potential for abuse. Providers of scheduled substances (physicians, dentists, podiatrists, advanced practitioners) may have links to the distribution of these substances. They are required to have a DEA license and record prescription of scheduled drugs. This licensing prevents overprescribing and obligates providers to be wary of potential drug-seeking patients. The dispenser must also be aware of a patient's medication history and be mindful of the potential for polypharmacy if a patient seeks multiple providers. The current opioid epidemic is a time where federal oversight and interdisciplinary coordination have the potential to reduce harm to patients prescribed scheduled drugs drastically. It will, however, take further time and evaluation to know if drug scheduling actually reduces abuse, addiction, and overdose.[6][7][8][9][10]
Nursing, Allied Health, and Interprofessional Team Interventions
The healthcare team, e.g., physicians, nurses, pharmacists, etc., need to work together to address the proper medical use of controlled substances, e.g., pain control pharmacotherapy. The healthcare team should schedule their patients for routine follow-up visits that include a history and physical exam to monitor for adverse drug effects and drug misuse. Monitoring for signs of drug misuse is a very important responsibility for the healthcare team because of the epidemic rates of drug misuse worldwide, e.g., the USA, which leads to death because of respiratory depression as in the case of opioid analgesics. Methods for monitoring drug abuse as well as drug diversion include the following examples: assessment surveys, state prescription drug monitoring programs, urine screening, adherence check-lists, motivational counseling, and dosage form counting, e.g., tablet counting.
(Click Image to Enlarge)
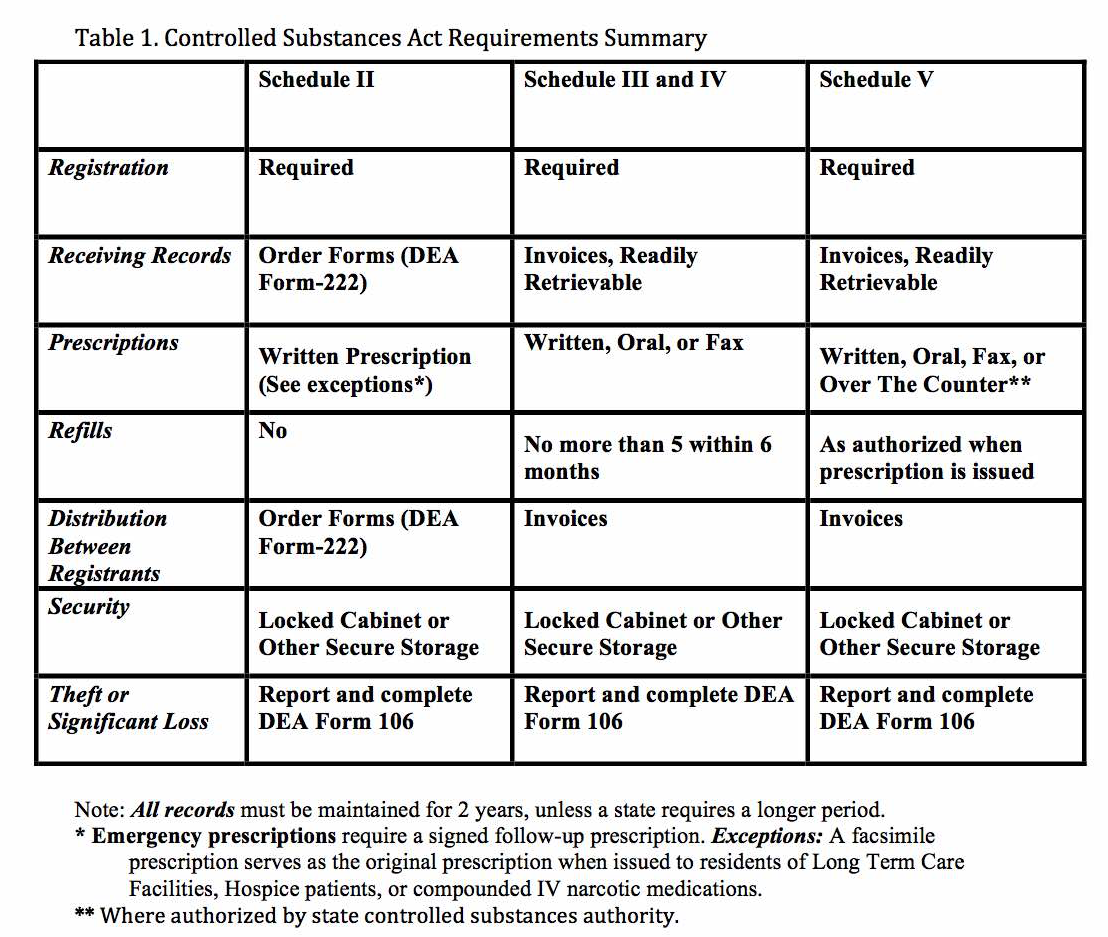
Controlled Substances Act Summary Table
Adapted from Department of Justice website https://www.deadiversion.usdoj.gov/
(Click Image to Enlarge)
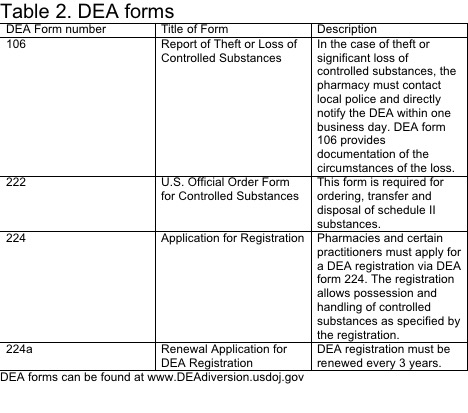
DEA forms
Adapted from https://www.deadiversion.usdoj.gov/, the website is work of the U.S. Government and is not subject to copyright protection in the United States.