Telangiectatic Osteosarcoma
- Article Author:
- Faten Limaiem
- Article Author:
- James Kuhn
- Article Editor:
- Karam Khaddour
- Updated:
- 10/16/2020 6:17:03 PM
- For CME on this topic:
- Telangiectatic Osteosarcoma CME
- PubMed Link:
- Telangiectatic Osteosarcoma
Introduction
Telangiectatic osteosarcoma is a rare high-grade malignant neoplasm, accounting for less than 4% of all cases of osteosarcoma.[1] It is a rare variant of osteosarcoma characterized by distinctive radiographic, gross, and microscopic features. It is a bone-forming tumor that mimics radiologically and microscopically aneurysmal bone cyst.
Etiology
The exact etiology of telangiectatic osteosarcoma is still unknown, and so are the predisposing factors. However, some anecdotal reports described genetic components due to the presence of the disease in family members.
Epidemiology
The mean age at presentation of telangiectatic osteosarcoma is 17.5 years (range: 15 to 20 years) with a male to female ratio of 2 to 1.[1] The distal femoral metaphysis is the single most common anatomic site (42%) followed by the proximal tibia (17%), the proximal humerus (9%), and the proximal femur (8%). Uncommon sites of telangiectatic osteosarcoma include the scapula, the ribs, the sternum, the innominate bone, the cranial vault, and the mandible. Telangiectatic osteosarcoma of the spine represents 2% of all cases of primary vertebral osteosarcomas.[2] Extra-osseous telangiectatic osteosarcoma is rare with telangiectatic osteosarcoma arising in the soft tissues of the thigh, the forearm, and popliteal fossa.[3]
Pathophysiology
Histogenesis
Telangiectatic osteosarcoma is presumed to derive from either transformed osteoblasts or stem cells of mesenchymal origin. Angiosarcomatous features present in addition to osteoblast-like and fibroblast-like cells at the ultrastructural level. Tight intercellular junctions, Weibel-Palade bodies, and pinocytic vesicles are visible within the cell cytoplasm. These features suggest that telangiectatic osteosarcoma derives from multipotential stem cells of mesenchymal origin.[4][1][5]
Cytogenetics
Only seven cases of telangiectatic osteosarcoma to date to date have had genetic studies. Cytogenetic analysis identified trisomy 3 in one case, and in three other tumors, more complex chromosomal changes were reported.[6][7] Metaphase CGH identified an average of 2.5 aberrations in two telangiectatic osteosarcomas and array CGH identified only three regional gains at 1q21-23.2, 1q25.2-31.1, and 7q21.13-21.2 in one tumor.[8] This suggests that telangiectatic tumors are genetically less complex than conventional osteosarcoma.
Histopathology
The resected surgical specimens of telangiectatic osteosarcoma must undergo meticulous sampling.[1] The complete face of the bone must be sampled to document the percentages of viable and necrotic tumor.[1]
Macroscopic Findings
Macroscopic examination reveals a hemorrhagic multicystic lesion filled with blood clots. Telangiectatic osteosarcomas have the classic description as ''a bag of blood.'' They are, by definition, composed of approximately 90% cystic components before treatment.[9] A fleshy sarcomatous component is typically not present. The cystic spaces can vary considerably in size and may occasionally measure several centimeters in diameter. More often, there is a mixture of large cystic and spongy areas. The spongy areas represent tissue honeycombed with smaller cysts that measure up to several millimeters in size. The borders of the lesion are usually well-demarcated, but often there are features of invasive growth with extensive irregular cortical erosion, complete disruption of cortical continuity, and invasion of soft tissue.
Microscopic Findings
Histologically, telangiectatic osteosarcoma is composed of blood-filled or empty cystic spaces resembling aneurysmal bone cyst. The septa are populated by pleomorphic cells with important nuclear hyperchromasia and also contain osteoclast-like giant cells. Osteoid formation is usually focal and confluent. Because telangiectatic osteosarcoma is sometimes not adequately sampled by core-needle biopsy due to its lytic and cystic nature, cellular atypia and osteoid formation may be absent, which may lead to misdiagnosis.[1] Misdiagnoses often delay accurate diagnoses and appropriate treatments, which may negatively influence patient prognosis.[10]
Immunochemistry
No immunohistochemical studies are useful in the diagnosis of telangiectatic osteosarcoma.
History and Physical
There is no difference in the clinical presentation of telangiectatic and conventional osteosarcoma. Local pain and/or soft tissue mass are the most common symptoms of telangiectatic osteosarcoma. Sometimes, the patients may present with a pathologic fracture.[11][12] Occasionally, a vascular bruit may be heard over the tumor.
Evaluation
Several imaging modalities are available for establishing the diagnosis of telangiectatic osteosarcoma. They include:
- Plain radiographs
- Computed tomography (CT)
- Magnetic resonance imaging (MRI)
Radiographic Findings
Telangiectatic osteosarcoma is typically a purely lytic lesion with a permeative destructive growth pattern. This rapidly growing tumor often expands the contour of bone and shows features of cortical disruption with minimal or no periosteal new bone formation. The massive expansile growth pattern of telangiectatic osteosarcoma can superficially simulate aneurysmal bone cyst. Telangiectatic osteosarcoma can have a deceptively innocent radiographic appearance with sharply demarcated margins, simulating a benign bone cyst. MRI best documents the multilocular cystic nature of the lesion and the so-called fluid level sign.[13] T1-weighted MRI shows heterogeneous low signal intensity, and T2-weighted images show high signal intensity with several cystic foci, fluid levels, and an extra-skeletal extension of the tumor, similar to an aneurysmal cyst, but with irregular walls, septae, and nodular and solid components.[14]
Criteria for the Diagnosis of Telangiectatic Osteosarcoma
The criteria for the diagnosing telangiectatic osteosarcoma include[15]:
- Radiographically, a destructive, osteolytic tumor with little or no matrix mineralization or periosteal new bone formation
- Cystic, cavitary gross specimen with little solid tumor tissue and no areas of a dense bone
- Histologically, a tumor with single or multiple cystic cavities, containing blood or necrotic tissue, with septa composed of anaplastic tumor cells
The high level of alkaline phosphatase frequently seen in osteosarcoma is not a feature of telangiectatic osteosarcoma.
Treatment / Management
Patients with telangiectatic osteosarcoma receive neo-adjuvant chemotherapy and, when possible, limb-sparing surgery.[16] The extent of surgery depends on the size, the location, and response to the neoadjuvant therapy. Adjuvant chemotherapy can offer some advantage if metastatic disease is present.
Differential Diagnosis
- Aneurysmal bone cyst
- Giant cell tumor of bone
- Brodie abscess
- Blood clot
- Malignant fibrous histiocytoma
- Fibrosarcoma
Treatment Planning
Chemotherapeutic protocols for telangiectatic osteosarcoma are similar to those of conventional osteosarcoma. Patients will have two to six cycles of chemotherapy administered before surgery. The common chemotherapeutic agents used include cisplatin, carboplatin, methotrexate, doxorubicin, and ifosfamide.[17] Among these, at least two agents need inclusion in a dual-drug therapy regimen. The effect of chemotherapy on telangiectatic osteosarcoma must undergo reassessment.
Prognosis
Telangiectatic osteosarcoma usually shows a better response to chemotherapy than conventional osteosarcoma. Survival rates with current chemotherapy protocols are within the range of 65% after 5 years.[18] The pattern of metastatic spread of telangiectatic osteosarcoma is similar to that seen in conventional osteosarcoma.
Tumor necrosis greater than 95% is considered one of the most important prognostic factors.[19] Additionally, uninvolved neurovascular bundles and soft tissue and bone resection margins are essential for a favorable prognosis.[1]
Enhancing Healthcare Team Outcomes
Telangiectatic osteosarcoma is a rare and aggressive variant of osteosarcoma with distinctive radiological and pathological features. It poses diagnostic difficulties mainly with an aneurysmal bone cyst. Distinguishing between these two entities is vital since their management and prognosis differ significantly. Telangiectatic osteosarcoma is ideally managed by an interprofessional team that consists of orthopedists, oncologists, radiologists, pathologists, pharmacists, and specialty care nurses. Pharmacists review chemotherapeutic regimens, check for drug-drug interactions, and provide patient and family education. Specialty care oncology nurses administer chemotherapy, educate patients and their families, monitor for side effects, and provided feedback on the patient's condition to the team. [Level 5]
(Click Image to Enlarge)
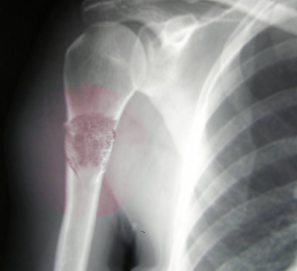
Telangiectactic osteosarcoma
Image courtesy S Bhimji MD